

Mirtazapine versus other antidepressive agents for depression
- PMID: 22161405
- PMCID: PMC4158430
- DOI: 10.1002/14651858.CD006528.pub2
Mirtazapine versus other antidepressive agents for depression
Abstract
Background: Mirtazapine has a unique mechanism of antidepressive action and is one of the commonly used antidepressants in clinical practice.
Objectives: The aim of the present review was to assess the evidence on the efficacy and acceptability of mirtazapine compared with other antidepressive agents in the acute-phase treatment of major depression in adults.
Search methods: We searched the Cochrane Collaboration Depression, Anxiety and Neurosis review group's specialised register (CCDANCTR), which includes relevant randomised controlled trials from the following bibliographic databases: The Cochrane Library (all years to April 2011), EMBASE, (1980 to July 2011) MEDLINE (1950 to July 2011) and PsycINFO (1974 to July 2011). Reference lists of the reports of relevant studies were checked and experts in the field contacted. The review was not limited to English-language articles.
Selection criteria: Randomised controlled trials (RCTs) allocating participants with major depression to mirtazapine versus any other antidepressive agent.
Data collection and analysis: Two authors independently checked eligibility and extracted data on an intention-to-treat basis. The primary outcome was response to treatment. The secondary outcomes included dropouts and individual adverse events.Meta-analyses were conducted using the random-effects model.
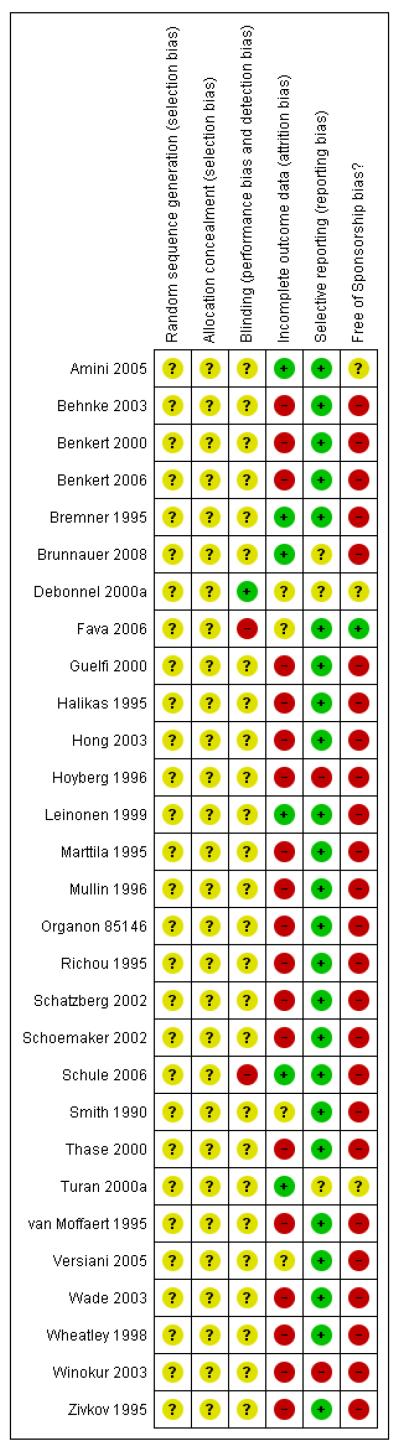
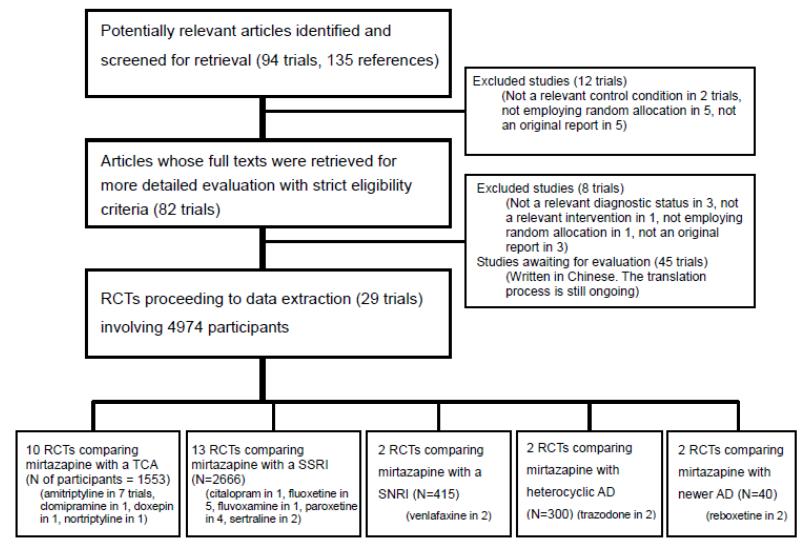
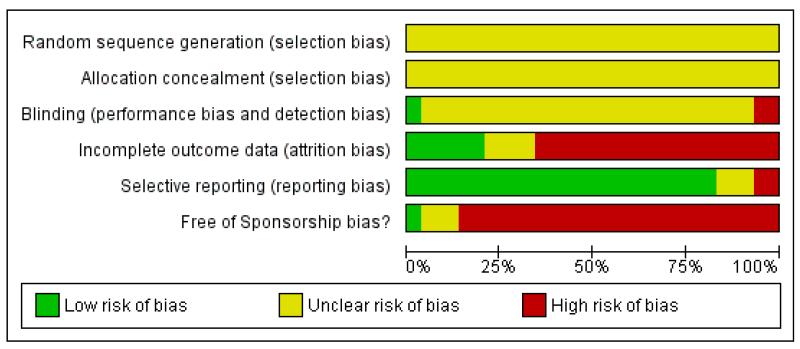
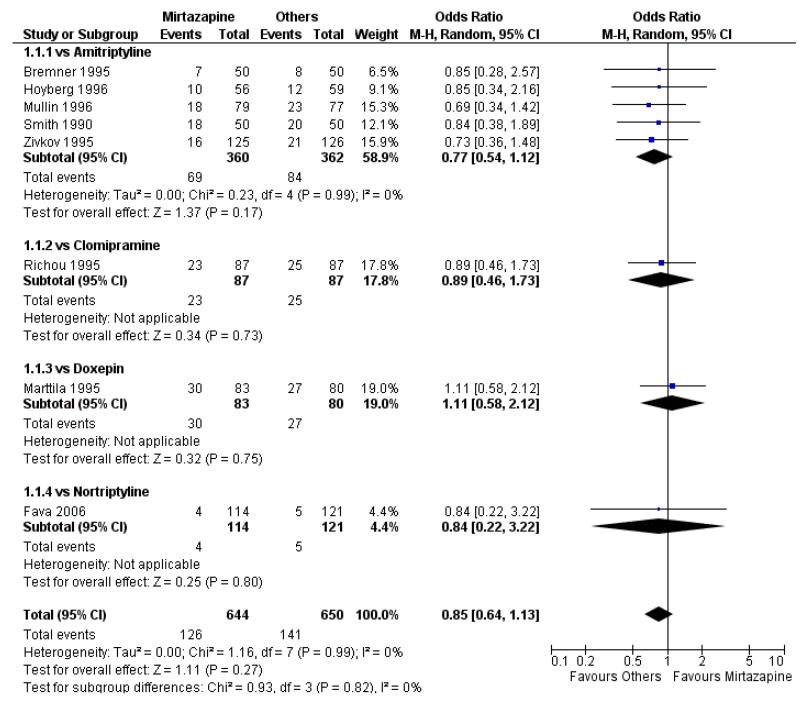
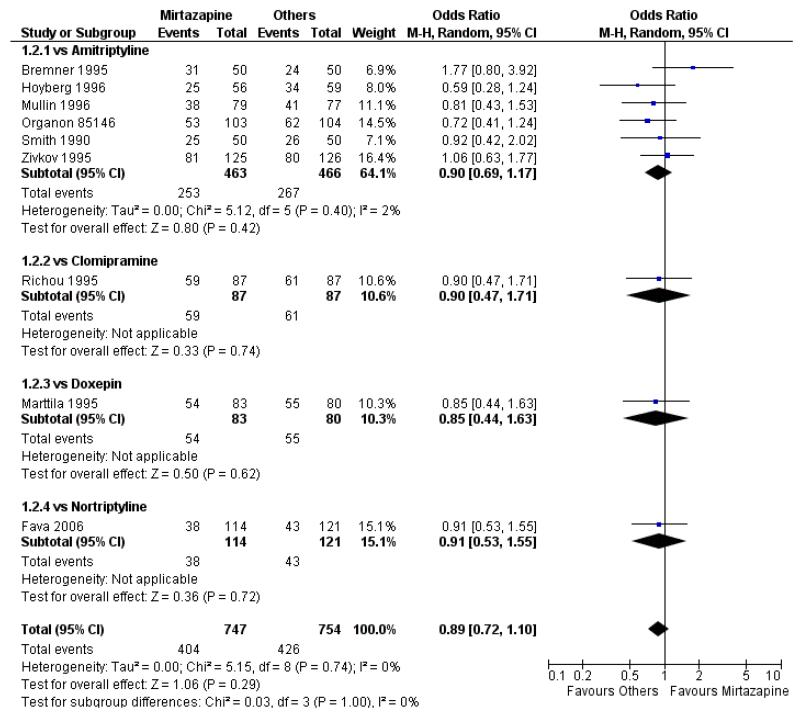
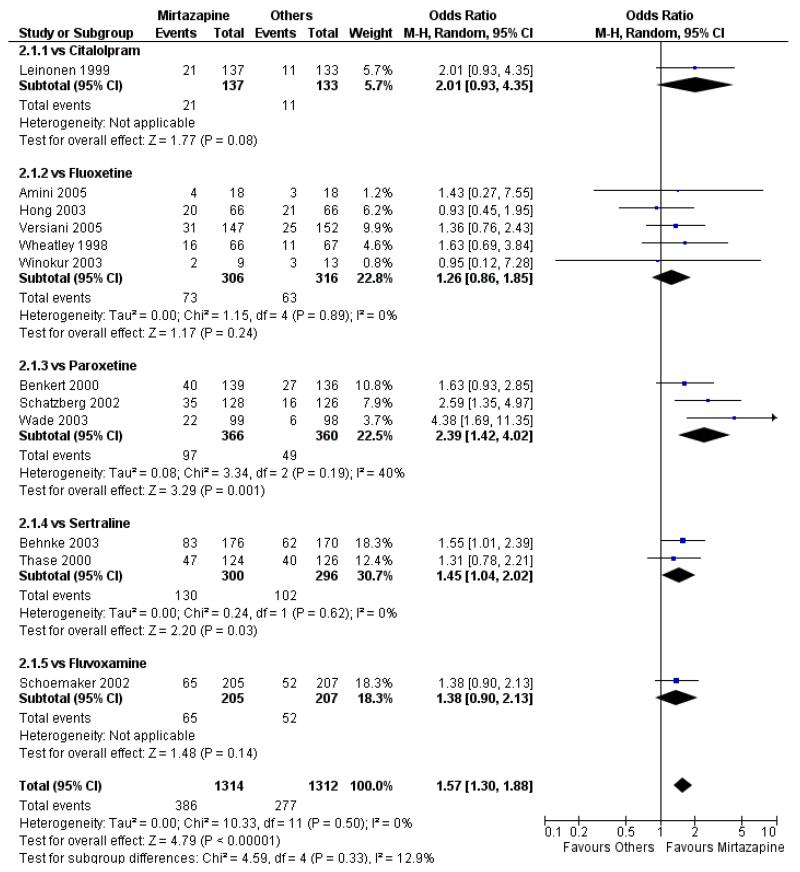
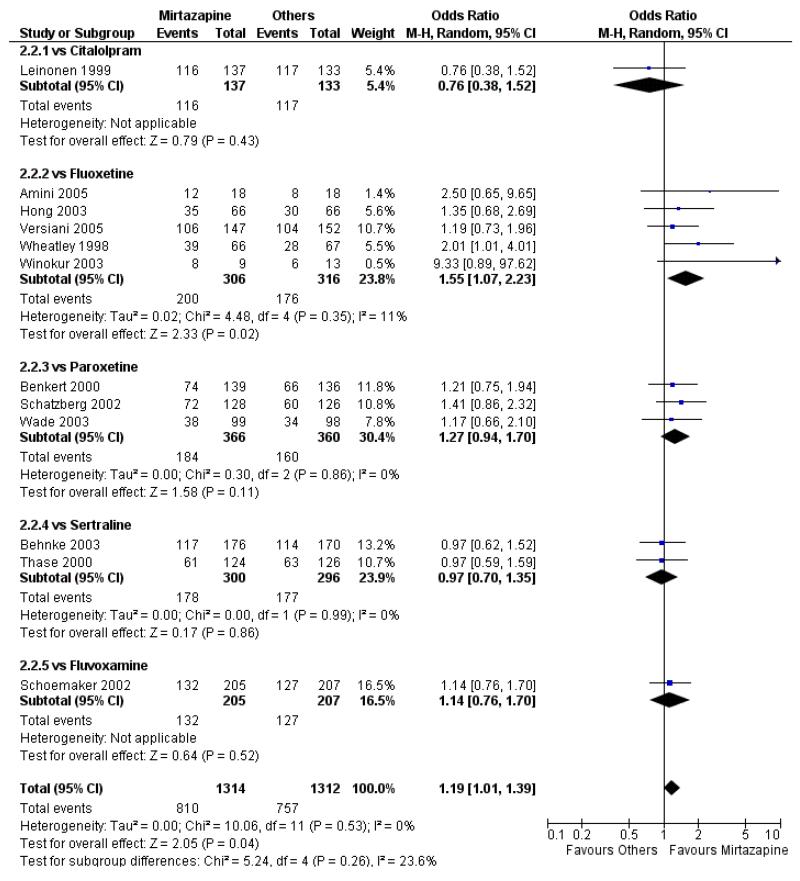
Main results: A total of 29 RCTs (n = 4974), mostly following up the participants for six weeks in outpatient clinics and inadequately reporting the risk of bias, were included. In comparison with tricyclic antidepressants (10 trials, n = 1553) there was no robust evidence to detect a difference between mirtazapine and tricyclics in terms of response at two weeks (odds ratio (OR) 0.85, 95% confidence interval (CI) 0.64 to 1.13) or at the end of acute-phase treatment (at 6 to 12 weeks) (OR 0.89, 95% CI 0.72 to 1.10). In comparison with selective serotonin reuptake inhibitors (SSRIs) (12 trials, n = 2626) mirtazapine was significantly more effective at two weeks (OR 1.57, 95% CI 1.30 to 1.88) and at the end of acute-phase treatment (OR 1.19, 95% CI 1.01 to 1.39). Mirtazapine was significantly more effective than a serotonin-noradrenaline reuptake inhibitor (venlafaxine only, two trials, n = 415) at two weeks (OR 2.29, 95% CI 1.45 to 3.59) and at the end of acute-phase treatment (OR 1.53, 95% CI 1.03 to 2.25).In terms of dropouts, there was no robust evidence to detect a difference between mirtazapine and other antidepressants. Mirtazapine was more likely to cause weight gain or increased appetite and somnolence than SSRIs but less likely to cause nausea or vomiting and sexual dysfunction.
Authors' conclusions: Some statistically significant and possibly clinically meaningful differences between mirtazapine and other antidepressive agents were found for the acute-phase treatment of major depression. Mirtazapine is likely to have a faster onset of action than SSRIs during the acute-phase treatment. Dropouts occur similarly in participants treated with mirtazapine and those treated with other antidepressants, although the adverse event profile of mirtazapine is unique.
Figures
References
References to studies included in this review
-
-
*
- Amini H, Aghayan S, Jalili SA, Akhondzadeh S, Yahyazadeh O, Pakravan-Nejad M. Comparison of mirtazapine and fluoxetine in the treatment of major depressive disorder: a double-blind, randomized trial. Journal of Clinical Pharmacy and Therapeutics. 2005;30(2):133–8. - PubMed
-
-
- Baker R, Schutte AJ. NR326 More rapid onset of sleep-improving effects with mirtazapine FDT versus sertraline; 158th Annual Meeting of the American Psychiatric Association; Atlanta, GA. 2005 May 21-26.2005.
-
-
*
- Behnke K, Sogaard J, Martin S, Bauml J, Ravindran AV, Agren H, et al. Mirtazapine orally disintegrating tablet versus sertraline: a prospective onset of action study. Journal of Clinical Psychopharmacology. 2003;23(4):358–64. Erratum appears in Journal of Clinical Psychopharmacology 2003;23 (6):682. - PubMed
-
-
-
*
- Benkert O, Szegedi A, Kohnen R. Mirtazapine compared with paroxetine in major depression. Journal of Clinical Psychiatry. 2000;61(9):656–63. - PubMed
-
-
-
*
- Benkert O, Szegedi A, Philipp M, Kohnen R, Heinrich C, Heukels A, et al. Mirtazapine orally disintegrating tablets versus venlafaxine extended release. Journal of Clinical Psychopharmacology. 2006;26(1):75–8. - PubMed
-
References to studies excluded from this review
-
-
*
- Blier P, Ward HE, Jacobs W, Herbert C, O’Hara SA, Pigott TA. Combining two antidepressants from treatment start: a preliminary analysis; New research program and abstracts, American Psychiatric Association 157th Annual Meeting; 2004.p. 157.
-
-
- Bruijn JA, Moleman P, Mulder PG, van den Broek WW. Comparison of 2 treatment strategies for depressed inpatients: Imipramine and lithium addition or mirtazapine and lithium addition. Journal of Clinical Psychiatry. 1998;59(12):657–63. - PubMed
-
- Bruijn JA, Moleman P, Mulder PG, van den Broek WW. Depressed in-patients respond differently to imipramine and mirtazapine. Pharmacopsychiatry. 1999;32(3):87–92. - PubMed
-
- Bruijn JA, Moleman P, Mulder PG, Van den Broek WW. Treatment of mood-congruent psychotic depression with imipramine. Journal of Affective Disorders. 2001;66:165–74. - PubMed
-
-
*
- Bruijn JA, Moleman P, Mulder PGH, van den Broek WW, van Hulst AM, van der Mast RC, et al. A double-blind, fixed blood-level study comparing mirtazapine with imipramine in depressed in-patients. Pharmacology. 1996;127:231–7. - PubMed
-
References to studies awaiting assessment
-
- Blier P, Gobbi G, Turcotte JE, de Montigny C, Boucher N, Hebert C, et al. Mirtazapine and paroxetine in major depression: A comparison of monotherapy versus their combination from treatment initiation. European Neuropsychopharmacology. 2009;19(7):457–65. - PubMed
-
- Catterson ML, Preskorn SH. Double-blind crossover study of mirtazapine, amitriptyline and placebo in patient with major depression; 149th Annual Meeting of the American Psychiatric Association; New York, NY. 1996 May 4-9.1996. p. 0157.
-
- Chang FW, Ma YP, Yan F, Wang CH. Comparative study of mirtazapine vs clomipramine in treatment of dysthymic disorder. Chinese Journal of New Drugs and Clinical Remedies. 2006;25(1):55–7.
-
- Chen X, Tan L, Zhao J, Li L, Chen Y. Randomized controlled clinical trials of remeron and fluoxetine in depressive patients. Chinese Journal of Clinical Psychology. 2002;10(2):100–2.
-
- Chen G, Gu G, Li C, et al. A study of mirtazapine and venlafaxine in the treatment of depression. Journal of Clinical Psychological Medicine. 2003;13(2):77–9.
Additional references
-
- Als-Nielsen B, Chen W, Gluud C, Kjaergard LL. Association of funding and conclusions in randomized drug trials: a reflection of treatment effect or adverse events? JAMA. 2003;290(7):921–8. - PubMed
-
- Anderson IM, Nutt DJ, Deakin JF. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 1993 British Association for Psychopharmacology guidelines. Journal of Psychopharmacology. 2000;14(1):3–20. - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders (DSM-III) 3rd Edition American Psychiatric Association; Washington, DC: 1980.
References to other published versions of this review
-
- Watanabe N, Omori IM, Nakagawa A, Cipriani A, Barbui C, McGuire H, et al. Mirtazapine versus other antidepressants in the acute-phase treatment of adults with major depression: systematic review and meta-analysis. Journal of Clinical Psychiatry. 2008;69(9):1404–15. - PubMed
-
- Watanabe N, Omori IM, Nakagawa A, Cipriani A, Barbui C, McGuire H, Churchill R, Furukawa TA, MANGA (Meta-Analysis of New Generation Antidepressants) Study Group Safety reporting and adverse-event profile of mirtazapine described in randomized controlled trials in comparison with other classes of antidepressants in the acute-phase treatment of adults with depression: systematic review and meta-analysis. CNS Drugs. 2010;24(1):35–53. DOI: 10.2165/11319480-000000000-00000. - PubMed
-
-
* Indicates the major publication for the study
-
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous