

Glycated hemoglobin and cancer incidence and mortality in the Atherosclerosis in Communities (ARIC) Study, 1990-2006
- PMID: 22161730
- PMCID: PMC3906204
- DOI: 10.1002/ijc.27394
Glycated hemoglobin and cancer incidence and mortality in the Atherosclerosis in Communities (ARIC) Study, 1990-2006
Abstract
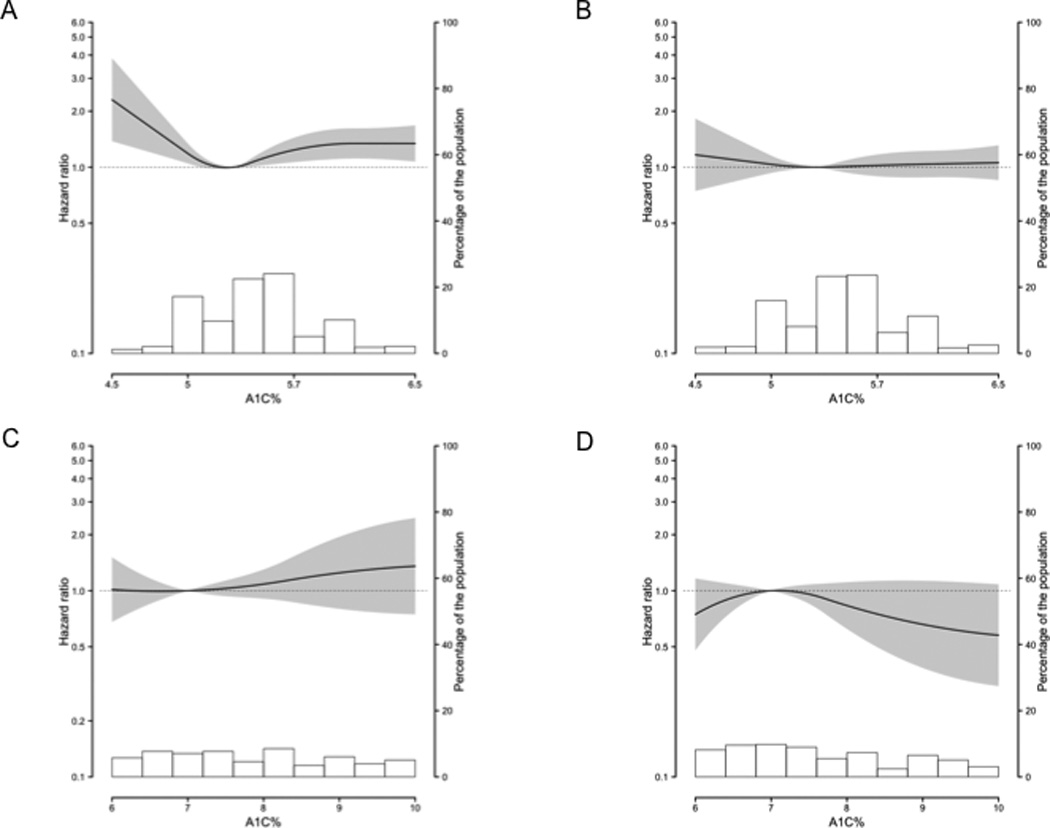
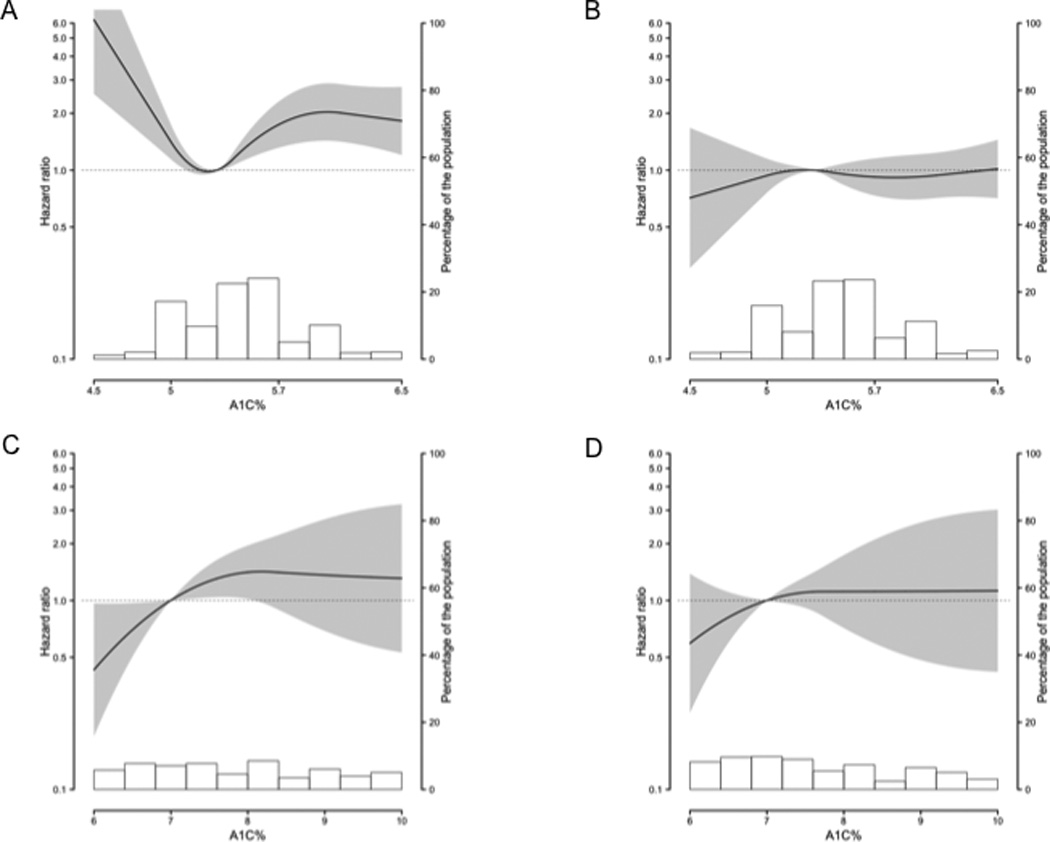
Diabetes is a risk factor for many cancers; chronic hyperglycemia is hypothesized to be, in part, explanatory. We evaluated the association between glycated hemoglobin, a time-integrated glycemia measure, and cancer incidence and mortality in nondiabetic and diabetic men and women. We conducted a prospective study of 12,792 cancer-free participants attending the second visit (1990-1992) of the Atherosclerosis Risk in Communities (ARIC) Study. We measured glycated hemoglobin in whole-blood samples using HPLC. Incident cancers were ascertained from registries and hospital records through 2006. We estimated multivariable-adjusted hazard ratios (HR) of cancer incidence and mortality for nondiabetic participants with values ≥ 5.7% (elevated), nondiabetic participants with <5.0% (low) and diabetic participants all compared with nondiabetic participants with 5.0-5.6% (normal). We ascertained 2,349 incident cancer cases and 887 cancer deaths. Compared with nondiabetic women with normal glycated hemoglobin, nondiabetic women with elevated values had an increased risk of cancer incidence (HR:1.24; 95% CI:1.07,1.44) and mortality (HR:1.58; 95% CI:1.23,2.05) as did diabetic women (incidence, HR:1.30; 95% CI:1.06,1.60, mortality, HR:1.96; 95% CI:1.40,2.76). Nondiabetic women with low values also had increased risk. Diabetic women with good glycemic control (<7.0%) had a lower cancer risk than those with higher values. Glycated hemoglobin in nondiabetic and diabetic men, and diabetes were not statistically significantly associated with total cancer risk. Our findings support the hypothesis that chronic hyperglycemia, even in the nondiabetic range, increases cancer risk in women. Maintaining normal glycated hemoglobin overall, and good glycemic control among diabetic adults, may reduce the burden of cancer, especially in women.
Copyright © 2011 UICC.
Figures
References
-
- Larsson SC, Wolk A. Diabetes mellitus and incidence of kidney cancer: a meta-analysis of cohort studies. Diabetologia. 2011;54:1013–1018. - PubMed
-
- Friberg E, Orsini N, Mantzoros CS, Wolk A. Diabetes mellitus and risk of endometrial cancer: a meta-analysis. Diabetologia. 2007;50:1365–1374. - PubMed
-
- Giovannucci E, Michaud D. The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology. 2007;132:2208–2225. - PubMed
-
- Larsson SC, Mantzoros CS, Wolk A. Diabetes mellitus and risk of breast cancer: a meta-analysis. Int J Cancer. 2007;121:856–862. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC055016/HL/NHLBI NIH HHS/United States
- T32CA009314/CA/NCI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- N01 HC055018/HC/NHLBI NIH HHS/United States
- P30 DK079637/DK/NIDDK NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- N01 HC055015/HC/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- T32 CA009314/CA/NCI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- K01 DK076595/DK/NIDDK NIH HHS/United States
- N01 HC055019/HC/NHLBI NIH HHS/United States
- T32 CA132670/CA/NCI NIH HHS/United States
- R21 DK080294/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
