

Clinical significance of quantifying Pneumocystis jirovecii DNA by using real-time PCR in bronchoalveolar lavage fluid from immunocompromised patients
- PMID: 22162560
- PMCID: PMC3264196
- DOI: 10.1128/JCM.06036-11
Clinical significance of quantifying Pneumocystis jirovecii DNA by using real-time PCR in bronchoalveolar lavage fluid from immunocompromised patients
Abstract
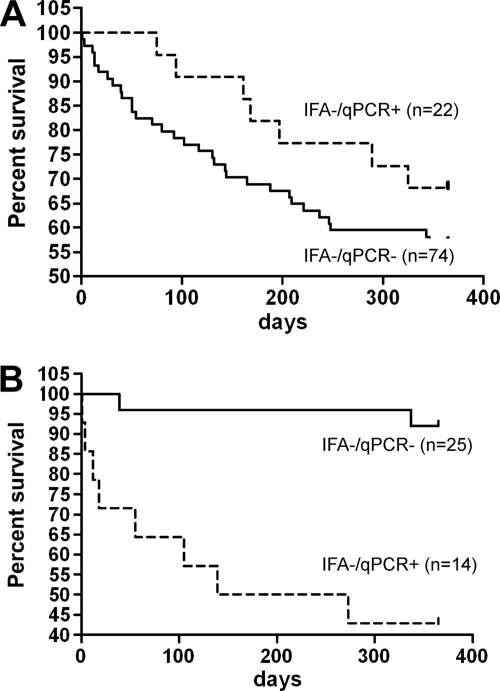
Quantitative PCR (qPCR) is more sensitive than microscopy for detecting Pneumocystis jirovecii in bronchoalveolar lavage (BAL) fluid. We therefore developed a qPCR assay and compared the results with those of a routine immunofluorescence assay (IFA) and clinical data. The assay included automated DNA extraction, amplification of the mitochondrial large-subunit rRNA gene and an internal control, and quantification of copy numbers with the help of a plasmid clone. We studied 353 consecutive BAL fluids obtained for investigation of unexplained fever and/or pneumonia in 287 immunocompromised patients. No qPCR inhibition was observed. Seventeen (5%) samples were both IFA and qPCR positive, 63 (18%) were IFA negative and qPCR positive, and 273 (77%) were both IFA and qPCR negative. The copy number was significantly higher for IFA-positive/qPCR-positive samples than for IFA-negative/qPCR-positive samples (4.2 ± 1.2 versus 1.1 ± 1.1 log(10) copies/μl; P < 10(-4)). With IFA as the standard, the qPCR assay sensitivity was 100% for ≥2.6 log(10) copies/μl and the specificity was 100% for ≥4 log(10) copies/μl. Since qPCR results were not available at the time of decision-making, these findings did not trigger cotrimoxazole therapy. Patients with systemic inflammatory diseases and IFA-negative/qPCR-positive BAL fluid had a worse 1-year survival rate than those with IFA-negative/qPCR-negative results (P < 10(-3)), in contrast with solid-organ transplant recipients (P = 0.88) and patients with hematological malignancy (P = 0.26). Quantifying P. jirovecii DNA in BAL fluids independently of IFA positivity should be incorporated into the investigation of pneumonia in immunocompromised patients. The relevant threshold remains to be determined and may vary according to the underlying disease.
Figures
References
-
- Alanio A, et al. 2011. Real-time PCR assay-based strategy for differentiation between active Pneumocystis jirovecii pneumonia and colonization in immunocompromised patients. Clin. Microbiol. Infect. 17: 1531–1537 - PubMed
-
- Arcenas RC, et al. 2006. A real-time polymerase chain reaction assay for detection of Pneumocystis from bronchoalveolar lavage fluid. Diagn. Microbiol. Infect. Dis. 54: 169–175 - PubMed
-
- Bandt D, Monecke S. 2007. Development and evaluation of a real-time PCR assay for detection of Pneumocystis jiroveci. Transpl. Infect. Dis. 9: 196–202 - PubMed
-
- Bollee G, et al. 2007. Clinical picture of Pneumocystis jiroveci pneumonia in cancer patients. Chest 132: 1305–1310 - PubMed
-
- Brancart F, Rodriguez-Villalobos H, Fonteyne PA, Peres-Bota D, Liesnard C. 2005. Quantitative TaqMan PCR for detection of Pneumocystis jiroveci. J. Microbiol. Methods 61: 381–387 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
