

Overcoming the challenges in the effective delivery of chemotherapies to CNS solid tumors
- PMID: 22163071
- PMCID: PMC3234205
- DOI: 10.4155/tde.10.22
Overcoming the challenges in the effective delivery of chemotherapies to CNS solid tumors
Abstract
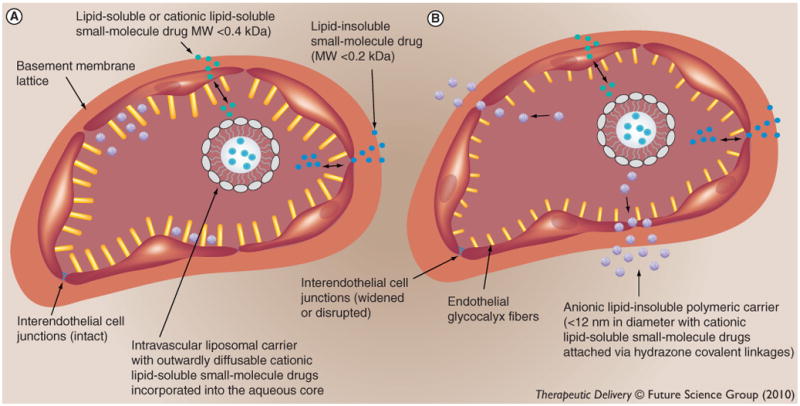
Locoregional therapies, such as surgery and intratumoral chemotherapy, do not effectively treat infiltrative primary CNS solid tumors and multifocal metastatic solid tumor disease of the CNS. It also remains a challenge to treat such CNS malignant solid tumor disease with systemic chemotherapies, although these lipid-soluble small-molecule drugs demonstrate potent cytotoxicity in vitro. Even in the setting of a 'normalized' tumor microenvironment, small-molecule drugs do not accumulate to effective concentrations in the vast majority of tumor cells, which is due to the fact that small-molecule drugs have short blood half-lives. It has been recently shown that drug-conjugated spherical lipid-insoluble nanoparticles within the 7-10 nm size range can deliver therapeutic concentrations of drug fraction directly into individual tumor cells following systemic administration, since these functionalized particles maintain peak blood concentrations for several hours and are smaller than the physiologic upper limit of pore size in the VEGF-derived blood capillaries of solid tumors, which is approximately 12 nm. In this article, the physiologic and ultrastructural basis of this novel translational approach for the treatment of CNS, as well as non-CNS, solid cancers is reviewed.
Conflict of interest statement
Figures
References
-
- Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med. 1990;322(8):494–500. - PubMed
-
- Weil RJ, Lonser RR, DeVroom HL, Wanebo JE, Oldfield EH. Surgical management of brainstem hemangioblastomas in patients with von Hippel-Lindau disease. J Neurosurg. 2003;98(1 Suppl):95–105. - PubMed
-
- Moss JM, Choi CY, Adler JR, Jr, Soltys SG, Gibbs IC, Chang SD. Stereotactic radiosurgical treatment of cranial and spinal hemangioblastomas. Neurosurgery. 2009;65(1):79–85. - PubMed
-
- Wohrer A, Waldhor T, Heinzl H, et al. The Austrian brain tumour registry: a cooperative way to establish a population-based brain tumour registry. J Neurooncol. 2009;95(3):401–411. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources