

Comparison of hip and knee strength and neuromuscular activity in subjects with and without patellofemoral pain syndrome
- PMID: 22163090
- PMCID: PMC3230156
Comparison of hip and knee strength and neuromuscular activity in subjects with and without patellofemoral pain syndrome
Abstract
Purpose/background: Historically, patellofemoral pain syndrome (PFPS) has been viewed exclusively as a knee problem. Recent findings have suggested an association between hip muscle weakness and PFPS. Altered neuromuscular activity about the hip also may contribute to PFPS; however, more limited data exist regarding this aspect. Most prior investigations also have not concurrently examined hip and knee strength and neuromuscular activity in this patient population. Additional knowledge regarding the interaction between hip and knee muscle function may enhance the current understanding of PFPS. The purpose of this study was to compare hip and knee strength and electromyographic (EMG) activity in subjects with and without PFPS.
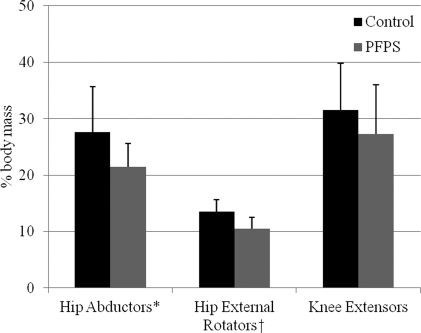
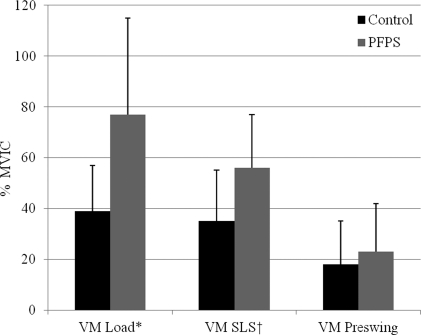
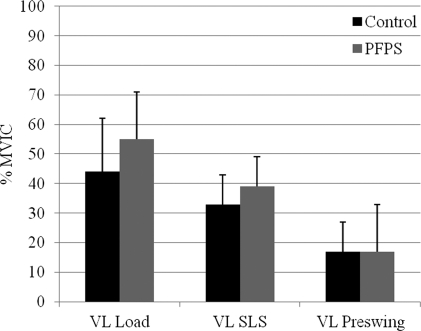
Methods: Eighteen females with PFPS and 18 matched controls participated in this study. First, surface EMG electrodes were donned on the gluteus medius, vastus medialis, and vastus lateralis. Strength measures then were taken for the hip abductors, hip external rotators, and knee extensors. Subjects completed a standardized stair-stepping task to quantify muscle activation amplitudes during the loading response, single leg stance, and preswing intervals of stair descent as well as to determine muscle onset timing differences between the gluteus medius and vastii muscles and between the vastus medialis and vastus lateralis at the beginning of stair descent.
Results: Females with PFPS demonstrated less strength of the hip muscles. They also generated greater EMG activity of the gluteus medius and vastus medialis during the loading response and single leg stance intervals of stair descent. No differences existed with respect to onset activation of the vastus medialis and vastus lateralis. All subjects had a similar delay in gluteus medius onset activation relative to the vastii muscles.
Conclusion: Rehabilitation should focus on quadriceps and hip strengthening. Although clinicians have incorporated gluteus medius exercise in rehabilitation programs, additional attention to the external rotators may be useful.
Level of evidence: 4.
Keywords: gluteus medius; knee; patella; surface electromyography.
Figures




References
-
- Heinjes EBerger MYBierma-Zeinstra SMABernsen RMDVerhaar JANKoes BW. Exercise therapy for patellofemoral pain syndrome. The Cochrane Library. Vol 1 Chichester, UK: John Wiley & Sons, Ltd.; 2004
-
- Witvrouw EWerner SMikkelsen CVan Tiggelen DVanden Berghe LCerulli G. Clinical classification of patellofemoral pain syndrome: guidelines for non-operative treatment. Knee Surg Sports Traumatol Arthrosc. 2005;13:122–130 - PubMed
-
- Fulkerson JP. Diagnosis and treatment of patients with patellofemoral pain. Am J Sports Med. 2002;30(3):447–456 - PubMed
-
- Natri AKannus PJarvinen M. Which factors predict the long-term outcome in chronic patellofemoral pain syndrome? A 7-yr prospective follow-up study. Med Sci Sports Exer. 1998;30:1572–1577 - PubMed
-
- Malone TRDavies GJWalsh WM. Muscular control of the patella. Clin Sports Med. 2002;21(3):349–362 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials