

Origin of heart rate variability and turbulence: an appraisal of autonomic modulation of cardiovascular function
- PMID: 22163222
- PMCID: PMC3233900
- DOI: 10.3389/fphys.2011.00095
Origin of heart rate variability and turbulence: an appraisal of autonomic modulation of cardiovascular function
Abstract
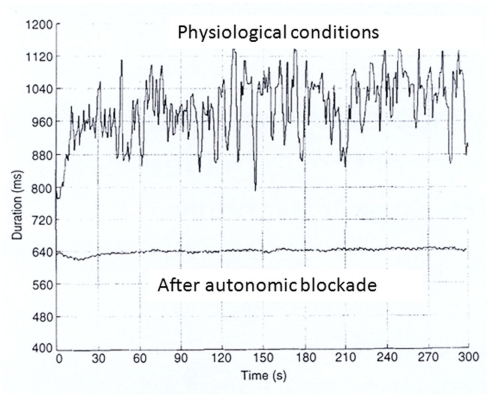
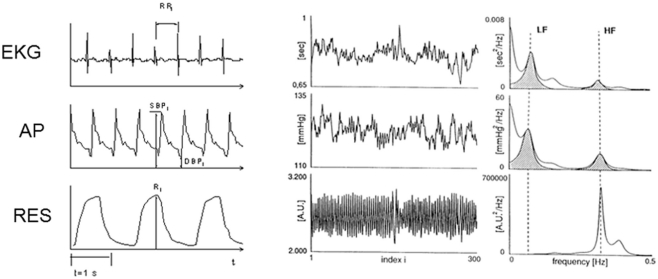
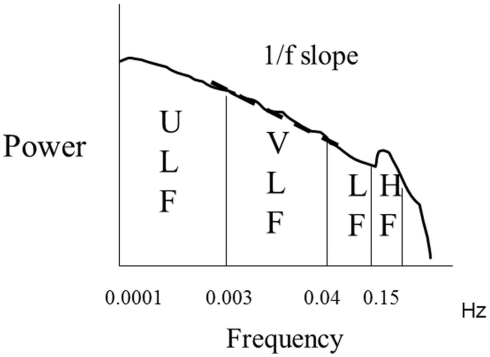
Heart period constantly changes on a beat to beat basis, due to autonomic influences on the sinoatrial node, and changes can be quantified as heart rate variability (HRV). In addition, after a premature ventricular beat, there are reproducible variations in RR interval, also due to baroreflex mediated autonomic influences on the sinoatrial node, that can be measured as heart rate turbulence (HRT). Impaired autonomic function as measured by HRV and HRT has proven to predict adverse outcomes in clinical settings. The ability of reduced HRV and HRT to predict adverse outcomes has been explained by their dependency on vagal mechanisms that could reflect an increased sympathetic and a reduced vagal modulation of sinus node, thus favoring cardiac electrical instability. Analysis of non-linear dynamics of HRV has also been utilized to describe the fractal like characteristic of the variability signal and proven effective in identify patients at risk for sudden cardiac death. Despite the clinical validity of these measures, it has also been evident that the relationship between neural input and sinus node responsiveness is extremely complex and variable in different clinical conditions. Thus, abnormal HRV or HRT on a clinical Holter recordings may reflect non-neural as well as autonomic mechanisms, and this also needs to be taken into account when interpreting any findings. However, under controlled conditions, the computation of the low and high frequency components of HRV and of their normalized powers or ratio seems capable of providing valid information on sympatho-vagal balance in normal subjects, as well as in most patients with a preserved left ventricular function. Thus, analysis of HRV does provide a unique tool to specifically assess autonomic control mechanisms in association with various perturbations. In conclusion, HRV measures are of substantial utility to identify patients with an increased cardiac mortality and to evaluate autonomic control mechanisms, but their ability to capture specific levels of autonomic control may be limited to controlled laboratory studies in relatively healthy subjects.
Keywords: autonomic modulation; baroreflex mechanisms; non-invasive evaluation of cardiac function; spectral analysis; sympathetic and vagal control.
Figures

References
-
- Bauer A., Barthel P., Müller A., Ulm K., Huikuri H., Malik M., Schmidt G. (2009). Risk prediction by heart rate turbulence and deceleration capacity in postinfarction patients with preserved left ventricular function retrospective analysis of 4 independent trials. J. Electrocardiol. 42, 597–60110.1016/j.jelectrocard.2009.07.013 - DOI - PubMed
-
- Bauer A., Malik M., Schmidt G., Barthel P., Bonnemeier H., Cygankiewicz I., Guzik P., Lombardi F., Müller A., Oto A., Schneider R., Watanabe M., Wichterle D., Zareba W. (2008). Heart rate turbulence: standards of measurement, physiological interpretation, and clinical use international society for Holter and noninvasive electrophysiology consensus. J. Am. Coll. Cardiol. 52, 1353–136510.1016/j.jacc.2008.07.041 - DOI - PubMed
-
- Bigger J. T., Fleiss J., Steinman R. C., Rolnitzky L. M., Kleiger R. E., Rottman J. N. (1992). Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 85, 164–171 - PubMed