

MRI findings for frozen shoulder evaluation: is the thickness of the coracohumeral ligament a valuable diagnostic tool?
- PMID: 22163326
- PMCID: PMC3233594
- DOI: 10.1371/journal.pone.0028704
MRI findings for frozen shoulder evaluation: is the thickness of the coracohumeral ligament a valuable diagnostic tool?
Abstract
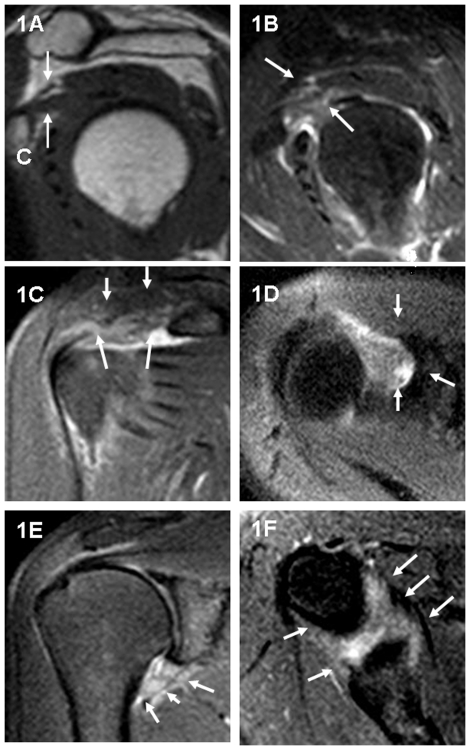
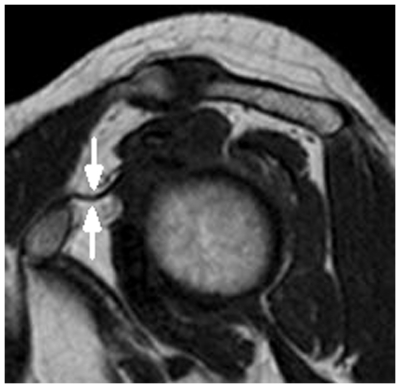
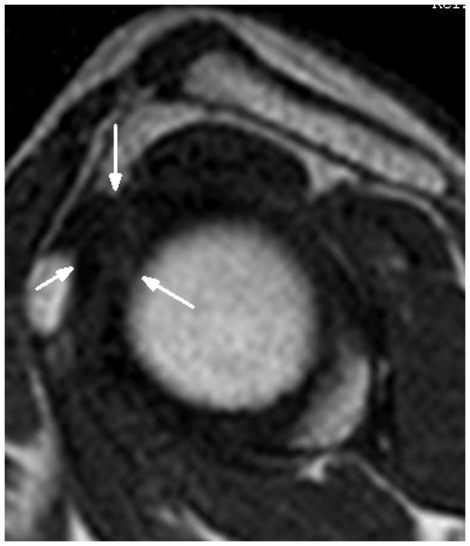
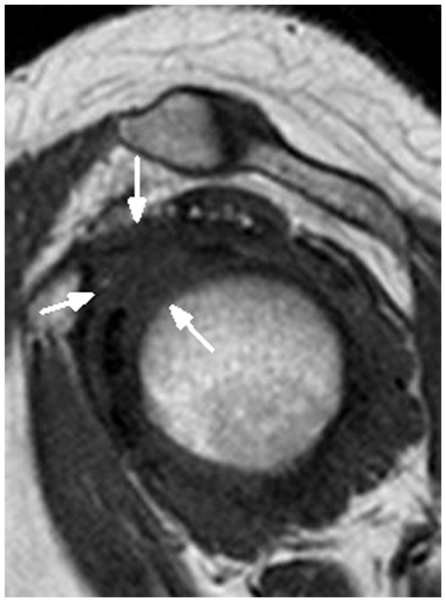
Background: Recent studies have demonstrated that the coracohumeral ligament (CHL) is shortened and thickened in a frozen shoulder. We analyzed the rate in CHL visualization between patients with frozen shoulder and normal volunteers using Magnetic Resonance Imaging (MRI) to determine the CHL thickness in the patients with a frozen shoulder.
Methods and findings: There were 72 shoulder joints in 72 patients (50 femles and 22 males with a mean age of 53.5 years) with clinical evidence and MR imaging evidence of frozen shoulder. These were prospectively analyzed to identify and measure the maximum thickness of the CHL. The control group, which included 120 shoulder joints in 60 normal volunteer individuals (30 females and 30 males with a mean age of 50.5 years) was also referred for MR imaging. A chi-square test was used to analyze the data of the rate of CHL visualization between the patients with frozen shoulder and the control group. A two-way ANOVA was used to analyze the mean maximal thickness of CHL. The CHL was visualized in 110 out of 120 shoulders in the control group (91.7%), and in 57 out of 72 shoulders for the frozen shoulder group (79.2%), there was significant difference, using a chi-square test (P<0.05). The CHL was not visualized in 10 out of 120 shoulders in the control group (8.3%), and 15 out of 72 shoulders in the frozen shoulder group (20.8%), there was a significant difference (P<0.05). The CHL thickness (3.99±1.68 mm) in the patients with frozen shoulder was significantly greater than that thickness (3.08±1.32 mm) in the control group, using a two-way ANOVA (P<0.001). The CHL thickness (3.52±1.52 mm, n = 97) in the female shoulders was no significantly greater than that thickness (3.22±1.49 mm, n = 70) in the male shoulders, using a two-way ANOVA (P>0.05).
Conclusions: MR Imaging is a satisfactory method for CHL depiction, and a thickened CHL is highly suggestive of frozen shoulder.
Conflict of interest statement
Figures
References
-
- Codman EA. Tendinitis of the short rotators. In: Codman EA, editor. Rupture of the supraspinatus tendon and other lesions on or about the subacromial bursa. Boston, Mass: Thomas Todd; 1934.
-
- Neviaser JS. Adhesive capsulitis of the shoulder: a study of the pathological findings in periarthritis of the shoulder. J Bone Joint Surg Am. 1945;27:211–22.
-
- Matsen FA, Fu FH, Hawkins RJ. The shoulder: a balance of mobility and stability. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1993.
-
- Zuckerman J, Cuomo F, Rokito S. Definition and classification of frozen shoulder: a consensus approach. J Shoulder Elbow Surg. 1994;3:S72. - PubMed
-
- Sano H, Hatori M, Mineta M, Hosaka M, Itoi E. Tumors masked as frozen shoulders: a retrospective analysis. J Shoulder Elbow Surg. 2010;19:262–266. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
