

Electronic nose breathprints are independent of acute changes in airway caliber in asthma
- PMID: 22163399
- PMCID: PMC3230982
- DOI: 10.3390/s101009127
Electronic nose breathprints are independent of acute changes in airway caliber in asthma
Abstract
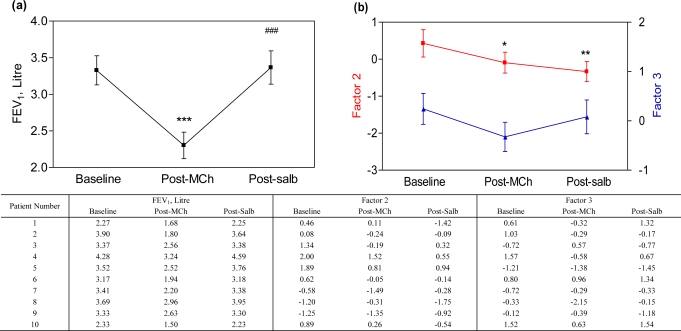
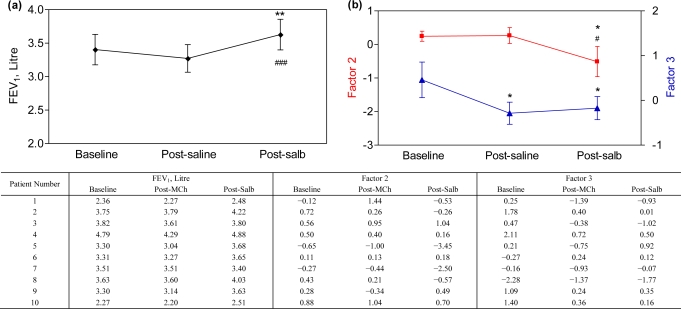
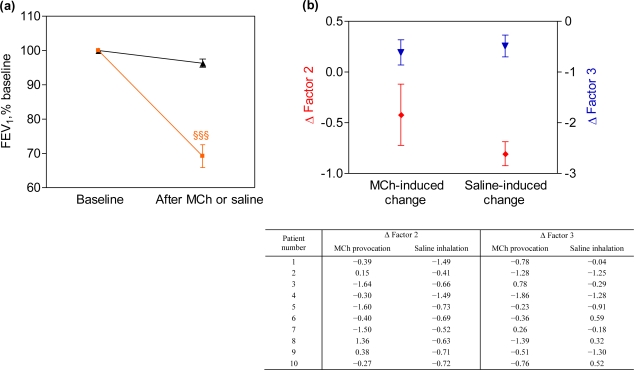
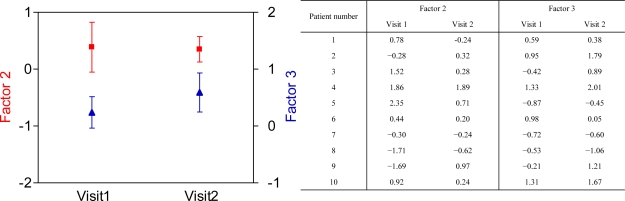
Molecular profiling of exhaled volatile organic compounds (VOC) by electronic nose technology provides breathprints that discriminate between patients with different inflammatory airway diseases, such as asthma and COPD. However, it is unknown whether this is determined by differences in airway caliber. We hypothesized that breathprints obtained by electronic nose are independent of acute changes in airway caliber in asthma. Ten patients with stable asthma underwent methacholine provocation (Visit 1) and sham challenge with isotonic saline (Visit 2). At Visit 1, exhaled air was repetitively collected pre-challenge, after reaching the provocative concentration (PC(20)) causing 20% fall in forced expiratory volume in 1 second (FEV(1)) and after subsequent salbutamol inhalation. At Visit 2, breath was collected pre-challenge, post-saline and post-salbutamol. At each occasion, an expiratory vital capacity was collected after 5 min of tidal breathing through an inspiratory VOC-filter in a Tedlar bag and sampled by electronic nose (Cyranose 320). Breathprints were analyzed with principal component analysis and individual factors were compared with mixed model analysis followed by pairwise comparisons. Inhalation of methacholine led to a 30.8 ± 3.3% fall in FEV(1) and was followed by a significant change in breathprint (p = 0.04). Saline inhalation did not induce a significant change in FEV(1), but altered the breathprint (p = 0.01). However, the breathprint obtained after the methacholine provocation was not significantly different from that after saline challenge (p = 0.27). The molecular profile of exhaled air in patients with asthma is altered by nebulized aerosols, but is not affected by acute changes in airway caliber. Our data demonstrate that breathprints by electronic nose are not confounded by the level of airway obstruction.
Keywords: airway caliber; bronchial asthma; bronchial provocation; electronic nose; exhaled breathprint; pattern recognition; volatile organic compounds.
Figures
Similar articles
-
Exhaled breath profiling enables discrimination of chronic obstructive pulmonary disease and asthma.Am J Respir Crit Care Med. 2009 Dec 1;180(11):1076-82. doi: 10.1164/rccm.200906-0939OC. Epub 2009 Aug 27. Am J Respir Crit Care Med. 2009. PMID: 19713445
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
External validation of exhaled breath profiling using an electronic nose in the discrimination of asthma with fixed airways obstruction and chronic obstructive pulmonary disease.Clin Exp Allergy. 2011 Oct;41(10):1371-8. doi: 10.1111/j.1365-2222.2011.03800.x. Epub 2011 Jul 7. Clin Exp Allergy. 2011. PMID: 21732998
-
Exhaled breath analysis by electronic nose in airways disease. Established issues and key questions.Clin Exp Allergy. 2013 Jul;43(7):705-15. doi: 10.1111/cea.12052. Clin Exp Allergy. 2013. PMID: 23786277 Review.
-
Breathomics and treatable traits for chronic airway diseases.Curr Opin Pulm Med. 2019 Jan;25(1):94-100. doi: 10.1097/MCP.0000000000000534. Curr Opin Pulm Med. 2019. PMID: 30325789 Review.
Cited by
-
An electronic-nose sensor node based on a polymer-coated surface acoustic wave array for wireless sensor network applications.Sensors (Basel). 2011;11(5):4609-21. doi: 10.3390/s110504609. Epub 2011 Apr 28. Sensors (Basel). 2011. PMID: 22163865 Free PMC article.
-
Breath Prints for Diagnosing Asthma in Children.J Clin Med. 2023 Apr 12;12(8):2831. doi: 10.3390/jcm12082831. J Clin Med. 2023. PMID: 37109167 Free PMC article.
-
The electronic nose technology in clinical diagnosis: A systematic review.Porto Biomed J. 2019 Jul 22;4(4):e42. doi: 10.1097/j.pbj.0000000000000042. eCollection 2019 Jul-Aug. Porto Biomed J. 2019. PMID: 31930178 Free PMC article. Review.
-
Assessment of the Portable C-320 Electronic Nose for Discrimination of Nine Insectivorous Bat Species: Implications for Monitoring White-Nose Syndrome.Biosensors (Basel). 2020 Feb 13;10(2):12. doi: 10.3390/bios10020012. Biosensors (Basel). 2020. PMID: 32069963 Free PMC article.
-
Are Volatile Organic Compounds Able to Identify Airflow Decline in Asthma?J Asthma Allergy. 2021 Jan 25;14:67-70. doi: 10.2147/JAA.S289278. eCollection 2021. J Asthma Allergy. 2021. PMID: 33531819 Free PMC article. No abstract available.
References
-
- National Heart and Lung Institute, National Institutes of Health USA, and the World Health Organization Global Initiative for Asthma. Dec, 2008. Update. Available at: http://www.ginasthma.org/ (accessed on 20 September 2010).
-
- Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding P, Wardlaw AJ, Pavord ID. Asthma exacerbations and sputum eosinophil counts: A randomised controlled trial. Lancet. 2002;360:1715–1721. - PubMed
-
- Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. New Engl. J. Med. 2005;352:2163–2173. - PubMed
-
- Moser B, Bodrogi F, Eibl G, Lechner M, Rieder J, Lirk P. Mass spectrometric profile of exhaled breath--field study by PTR-MS. Respir. Physiol. Neurobiol. 2005;145:295–300. - PubMed
-
- Van Berkel JJ, Dallinga JW, Moller GM, Godschalk RW, Moonen E, Wouters EF, Van Schooten FJ. Development of accurate classification method based on the analysis of volatile organic compounds from human exhaled air. J. Chromat. 2008;861:101–107. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
