

Effects of Intra-Arterial and Intravenous Iso-Osmolar Contrast Medium (Iodixanol) on the Risk of Contrast-Induced Acute Kidney Injury: A Meta-Analysis
- PMID: 22164156
- PMCID: PMC3222111
- DOI: 10.1159/000332384
Effects of Intra-Arterial and Intravenous Iso-Osmolar Contrast Medium (Iodixanol) on the Risk of Contrast-Induced Acute Kidney Injury: A Meta-Analysis
Abstract
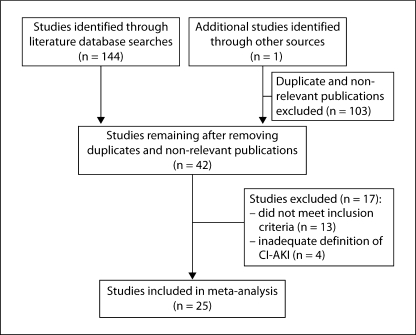
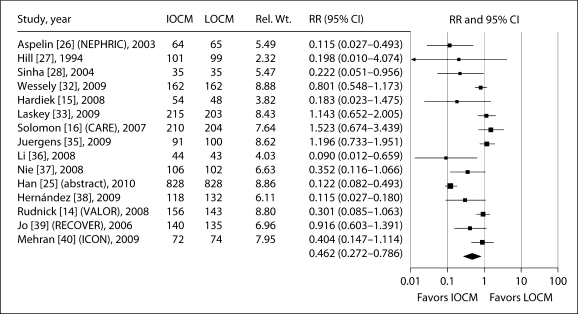
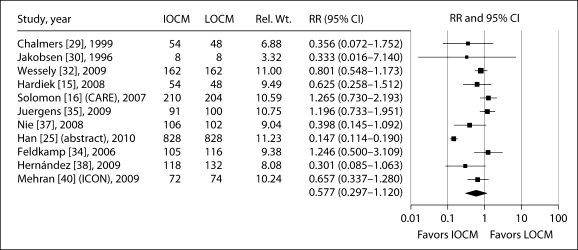
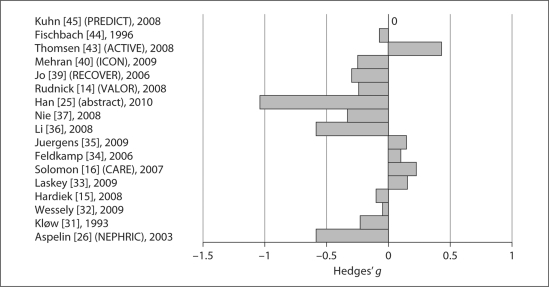
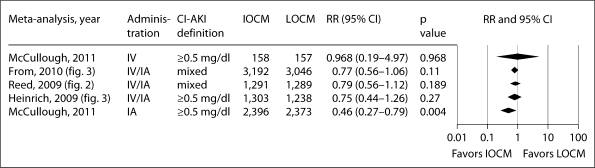
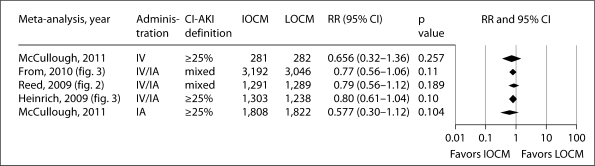
BACKGROUND: The iso-osmolar contrast agent iodixanol may be associated with a lower incidence of contrast-induced acute kidney injury (CI-AKI) than low-osmolar contrast media (LOCM), but previous meta-analyses have yielded mixed results. Objectives: To compare the incidence of CI-AKI between iodixanol and LOCM. METHODS: Studies were identified from literature searches to December 2009, clinicaltrials.gov, and conference abstracts from the past 2 years including 2010. Only prospective, randomized comparisons between iodixanol and LOCM with CI-AKI [increase in serum creatinine (sCr) ≥0.5 mg/dl or ≥25% from baseline, as defined in the trial] as a primary and/or secondary endpoint and a Jadad score ≥2 were included. A random-effects model was used to obtain pooled relative risks (RRs) for CI-AKI in analyses based on route of administration [intra-arterial (IA) or intravenous (IV)], definition of CI-AKI, and timing of sCr measurements. RESULTS: 145 potential articles were identified, of which 25 were included in the meta-analysis. Following IA administration (n = 19), the RR for CI-AKI (≥0.5 mg/dl definition) with iodixanol, compared with LOCM, was 0.462 [95% confidence interval (CI): 0.272-0.786, p = 0.004, 15 studies]. Using the ≥25% definition, there was a lower incidence of CI-AKI with iodixanol versus LOCM, but the difference was not statistically significant (RR: 0.577, 95% CI: 0.297-1.12, p = 0.104, 11 studies). In the IV trials, there was no significant difference in the incidence of CI-AKI using either definition (≥0.5 mg/dl definition: RR: 0.967, 95% CI: 0.188-4.972, p = 0.968, 3 trials; ≥25% definition: RR: 0.656, 95% CI: 0.316-1.360, p = 0.257, 4 trials). CONCLUSIONS: IA but not IV administration of iodixanol is associated with a significantly lower risk of CI-AKI than LOCM.
Figures
References
-
- Morcos SK. Contrast medium-induced nephrotoxicity. In: Dawson P, Cosgrove DO, Grainger RG, editors. Textbook of Contrast Media. Oxford: Isis Medical Media; 1999. pp. 135–148.
-
- Rihal CS, Textor SC, Grill DE, Berger PB, Ting HH, Best PJ, Singh M, Bell MR, Barsness GW, Mathew V, Garratt KN, Holmes DR., Jr Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105:2259–2264. - PubMed
-
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930–936. - PubMed
-
- McCullough PA, Adam A, Becker CR, Davidson C, Lameire N, Stacul F, Tumlin J, CIN Consensus Working Panel Risk prediction of contrast-induced nephropathy. Am J Cardiol. 2006;98:27K–36K. - PubMed
-
- Dangas G, Iakovou I, Nikolsky E, Aymong ED, Mintz GS, Kipshidze NN, Lansky AJ, Moussa I, Stone GW, Moses JW, Leon MB, Mehran R. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005;95:13–19. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous