

In vitro evaluation of gaseous microemboli handling of cardiopulmonary bypass circuits with and without integrated arterial line filters
- PMID: 22164448
- PMCID: PMC4679969
In vitro evaluation of gaseous microemboli handling of cardiopulmonary bypass circuits with and without integrated arterial line filters
Abstract
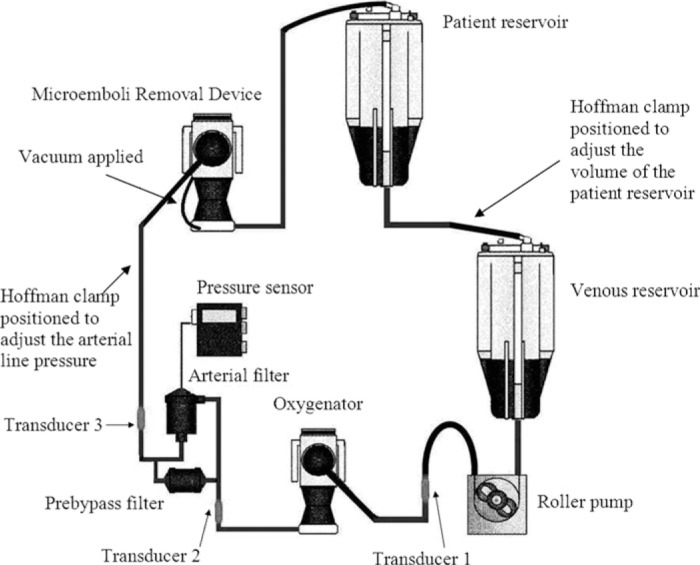
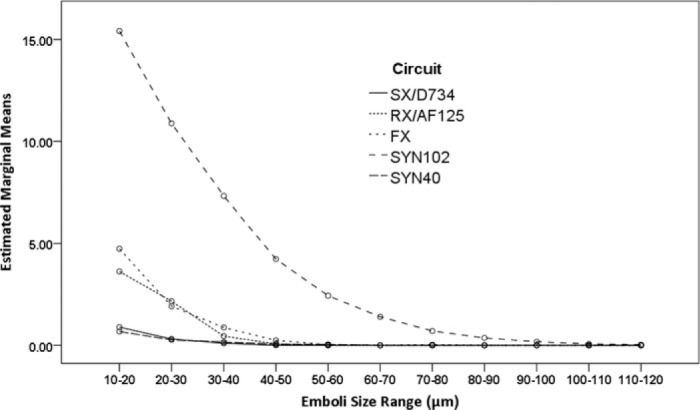
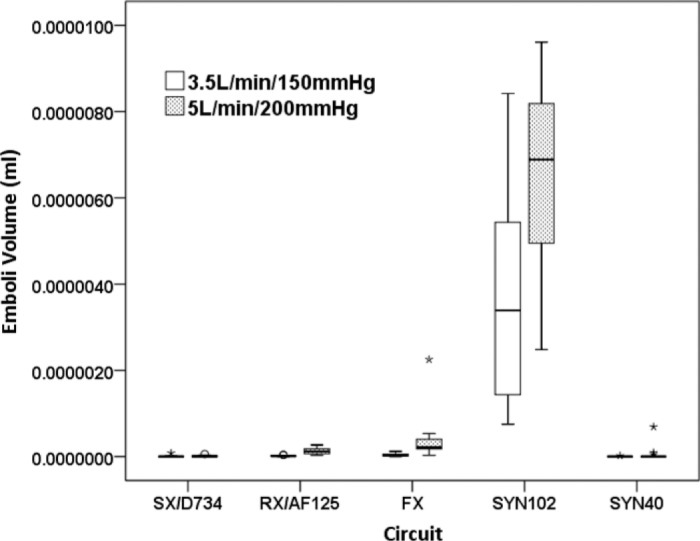
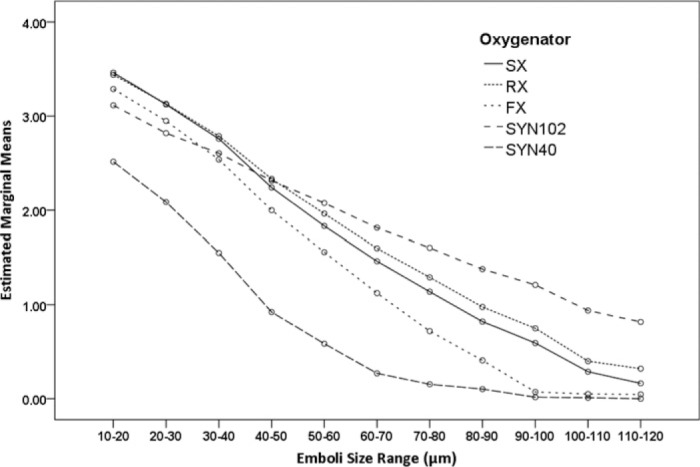
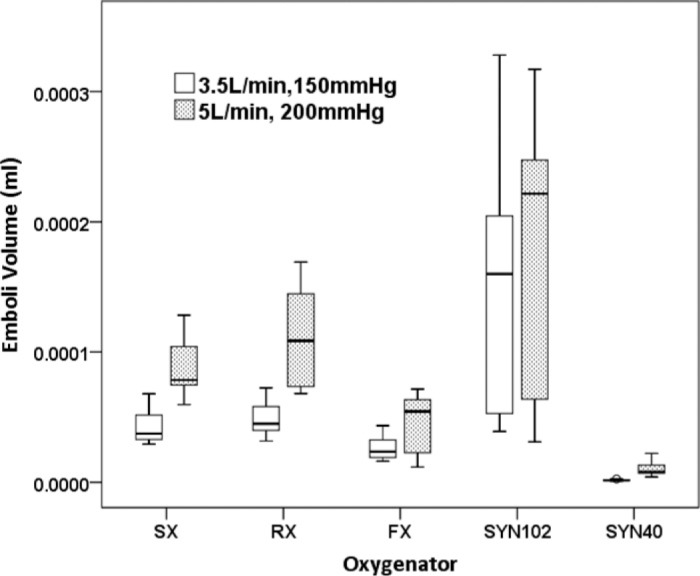
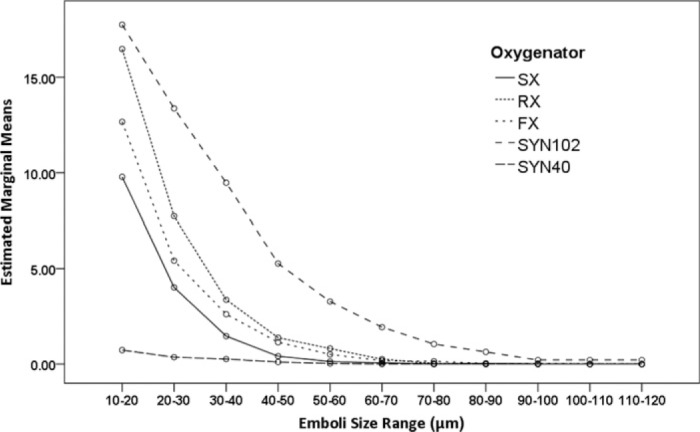
The delivery of gaseous microemboli (GME) by the cardiopulmonary bypass circuit should be minimized whenever possible. Innovations in components, such as the integration of arterial line filter (ALF) and ALFs with reduced priming volumes, have provided clinicians with circuit design options. However, before adopting these components clinically, their GME handling ability should be assessed. This study aims to compare the GME handling ability of different oxygenator/ALF combinations with our currently utilized combination. Five commercially available oxygenator/ALF combinations were evaluated in vitro: Terumo Capiox SX25RX and Dideco D734 (SX/D734),Terumo Capiox RX25R and AF125 (RX/AF125), Terumo FX25R (FX), Sorin Synthesis with 102 microm reservoir filter (SYN102), and Sorin Synthesis with 40 microm reservoir filter (SYN40). GME handling was studied by introducing air into the venous return at 100 mL/min for 60 seconds under two flow/ pressure combinations: 3.5 L/min, 150 mmHg and 5 L/min, 200 mmHg. Emboli were measured at three positions in the circuit using the Emboli Detection and Classification (EDAC) Quantifier and analyzed with the General Linear Model. All circuits significantly reduced GME. The SX/D734 and SYN40 circuits were most efficient in GME removal whilst the SYN102 handled embolic load (count and volume) least efficiently (p < .001). A greater number of emboli <70 microm were observed for the SYN102, FX and RX/AF125 circuits (p < .001). An increase in embolic load occurred with higher flow/pressure in all circuits (p < .001). The venous reservoir significantly influences embolic load delivered to the oxygenator (p < .001). The majority of introduced venous air was removed; however, significant variation existed in the ability of the different circuits to handle GME. Venous reservoir design influenced the overall GME handling ability. GME removal was less efficient at higher flow and pressure, and for smaller sized emboli. The clinical significance of reducing GME requires further investigation.
Conflict of interest statement
The senior author has stated that authors have reported no material, financial, or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures
Comment in
-
"See, feel, change".J Extra Corpor Technol. 2011 Sep;43(3):101-2. J Extra Corpor Technol. 2011. PMID: 22167841 Free PMC article. No abstract available.
References
-
- Barak M, Katz Y.. Microbubbles: Pathophysiology and clinical implications. Chest. 2005;128:2918–32. - PubMed
-
- Stump DA.. Embolic factors associated with cardiac surgery. Semin Cardiothorac Vasc Anesth. 2005;9:151–2. - PubMed
-
- Pugsley W, Klinger L, Paschalis C, Treasure T, Harrison M, Newman S.. The impact of microemboli during cardiopulmonary bypass on neuropsychological functioning. Stroke. 1994;25:1393–9. - PubMed
-
- Borger MA, Peniston CM, Weisel RD, Vasiliou M, Green RE, Feindel CM.. Neuropsychologic impairment after coronary artery bypass surgery. Effect of gaseous microemboli during perfusionist interventions. J Thorac Cardiovasc Surg. 2001;121:743–9. - PubMed
-
- Rodriguez RA, Williams KA, Babaev A, Rubens F, Nathan HJ.. Effect of perfusionist technique on cerebral embolization during cardiopulmonary bypass. Perfusion. 2005;20:3–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources