

In-vitro quantification of gaseous microemboli in two extracorporeal life support circuits
- PMID: 22164450
- PMCID: PMC4679971
In-vitro quantification of gaseous microemboli in two extracorporeal life support circuits
Abstract
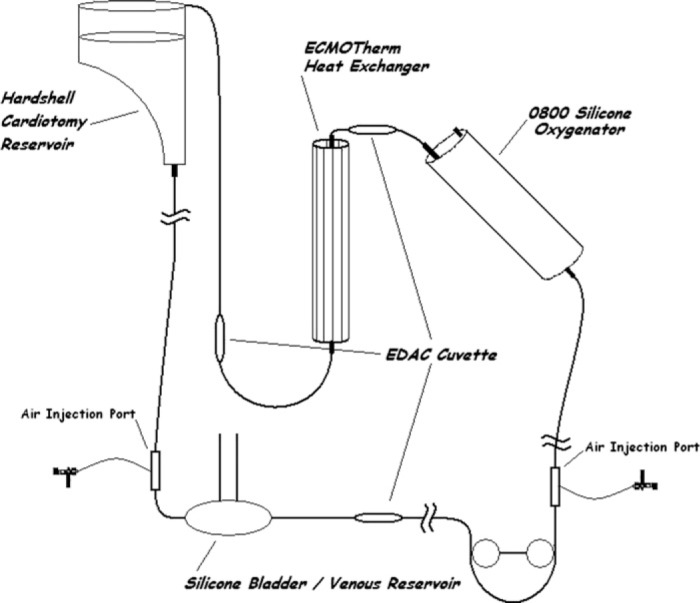
During the course of extracorporeal membrane oxygenation, patients are at constant risk of exposure to air emboli. Air emboli may enter the circuit during routine lab sampling, medication administration, air entrainment through the venous cannula, or via a circuit disruption. Circuit components have been designed and positioned to minimize the quantity of air that travels through the arterial line to the patient. The purpose of this study was to assess the air handling of a newer generation extracorporeal life support circuit. The extracorporeal life support circuit consisted of an open hard-shell venous reservoir, Better Bladder (BB14) or silicone bladder (R-14), and Quadrox D oxygenator or 0800 silicone oxygenator. Air emboli detection sensors were placed in the extracorporeal life support circuit: post bladder, post oxygenator, and post heat exchanger if applicable.Air was injected as a 1 mL/min for 5 minutes injection or as a single 5 mL bolus. Emboli detection was recorded continuously during and for 3 minutes post air injection at two blood flow rates (Qb) (.5 and 1.2 L/min). All tests were performed in triplicate with each condition. All tested components reduced the embolic volume transmitted through the circuit. The quantity of this reduction was dependent on both the Qb and the air injection condition. During this in-vitro testing, air emboli passing through any of the components tested was decreased. Furthermore, the emboli delivery was reduced post component with the slower Qb (.5 L/min).
Conflict of interest statement
The senior author has stated that authors have reported no material, financial, or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures







Comment in
-
"See, feel, change".J Extra Corpor Technol. 2011 Sep;43(3):101-2. J Extra Corpor Technol. 2011. PMID: 22167841 Free PMC article. No abstract available.
References
-
- Undar A, Ji B, Kunselman AR, Myers JL.. Detection and classification of gaseous microemboli during pulsatile and nonpulsatile perfusion in a simulated neonatal CPB model. ASAIO J. 2007;53:725–9. - PubMed
-
- Win KN, Wang S, Undar A.. Microemboli generation, detection and characterization during CPB procedures in neonates, infants, and small children. ASAIO J. 2008;54:486–90. - PubMed
-
- Schreiner RS, Rider AR, Myers JW, et al. Microemboli detection and classification by innovative ultrasound technology during simulated neonatal cardiopulmonary bypass at different flow rates, perfusion modes, and perfusate temperatures. ASAIO J. 2008;54:316–24. - PubMed
-
- Butler B.. Gaseous micro emboli: Concepts and considerations. J Extra Corpor Technol. 1983;15:148–55.
-
- Lynch JE, Riley JB.. Microemboli detection on extracorporeal bypass circuits. Perfusion. 2008;23:23–32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous