

Urticaria and angioedema
- PMID: 22165855
- PMCID: PMC3245442
- DOI: 10.1186/1710-1492-7-S1-S9
Urticaria and angioedema
Abstract
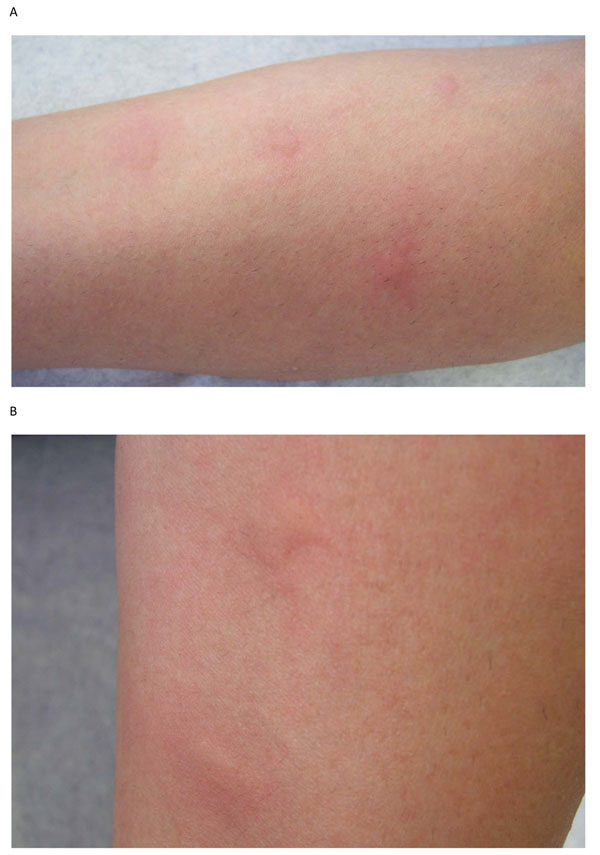
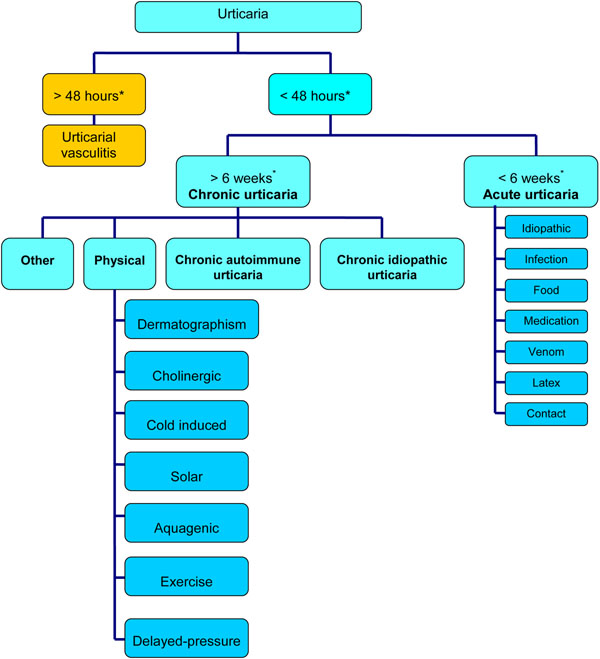
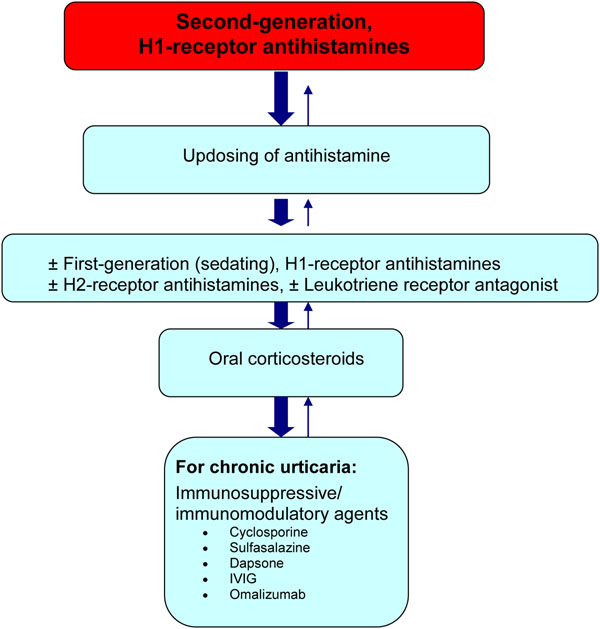
Urticaria (hives) is a common disorder that often presents with angioedema (swelling that occurs beneath the skin). It is generally classified as acute, chronic or physical. Second-generation, non-sedating H1-receptor antihistamines represent the mainstay of therapy for both acute and chronic urticaria. Angioedema can occur in the absence of urticaria, with angiotensin-converting enzyme (ACE) inhibitor-induced angioedema and idiopathic angioedema being the more common causes. Rarer causes are hereditary angioedema (HAE) or acquired angioedema (AAE). Although the angioedema associated with these disorders is often self-limited, laryngeal involvement can lead to fatal asphyxiation in some cases. The management of HAE and AAE involves both prophylactic strategies to prevent attacks of angioedema (i.e., trigger avoidance, attenuated androgens, tranexamic acid, and plasma-derived C1 inhibitor replacement therapy) as well as pharmacological interventions for the treatment of acute attacks (i.e., C1 inhibitor replacement therapy, ecallantide and icatibant). In this article, the authors review the causes, diagnosis and management of urticaria (with or without angioedema) as well as the work-up and management of isolated angioedema, which vary considerably from that of angioedema that occurs in the presence of urticaria.
Figures
References
-
- Powell RJ, Du Toit GL, Siddique N, Leech SC, Dixon TA, Clark AT, Mirakian R, Walker SM, Huber PA, Nasser SM. British Society for Allergy and Clinical Immunology (BSACI) BSACI guidelines for the management of chronic urticaria and angio-oedema. Clin Exp Allergy. 2007;37:631–650. doi: 10.1111/j.1365-2222.2007.02678.x. - DOI - PubMed
-
- Fonacier LS, Dreskin SC, Leung DY. Allergic skin diseases. J Allergy Clin Immunol. 2010;125(2 Suppl 2):S138–149. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
