

Mid- and long-term clinical results of surgical therapy in unicameral bone cysts
- PMID: 22165900
- PMCID: PMC3258224
- DOI: 10.1186/1471-2474-12-281
Mid- and long-term clinical results of surgical therapy in unicameral bone cysts
Abstract
Background: Unicameral (or simple) bone cysts (UBC) are benign tumours most often located in long bones of children and adolescents. Pathological fractures are common, and due to high recurrence rates, these lesions remain a challenge to treat. Numerous surgical procedures have been proposed, but there is no general consensus of the ideal treatment. The aim of this investigation therefore was to study the long-term outcome after surgical treatment in UBC.
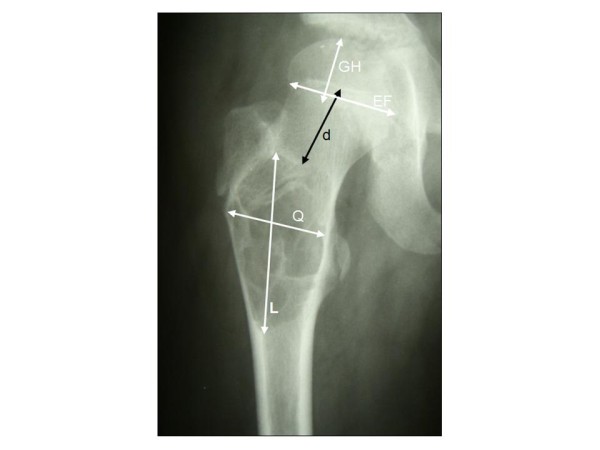
Methods: A retrospective analysis of 46 patients surgically treated for UBC was performed for short and mid-term outcome. Clinical and radiological outcome parameters were studied according to a modified Neer classification system. Long-term clinical information was retrieved via a questionnaire at a minimum follow-up of 10 years after surgery.
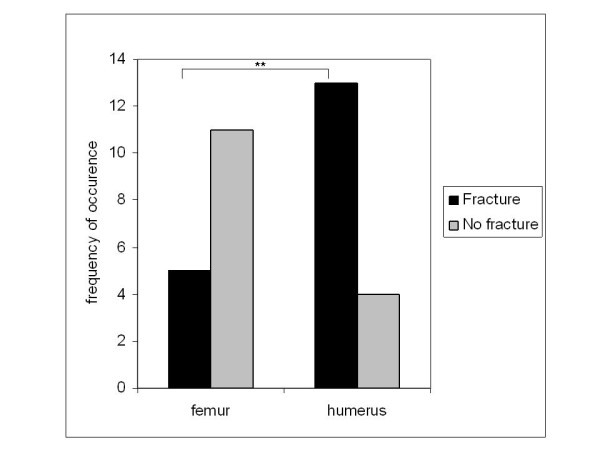
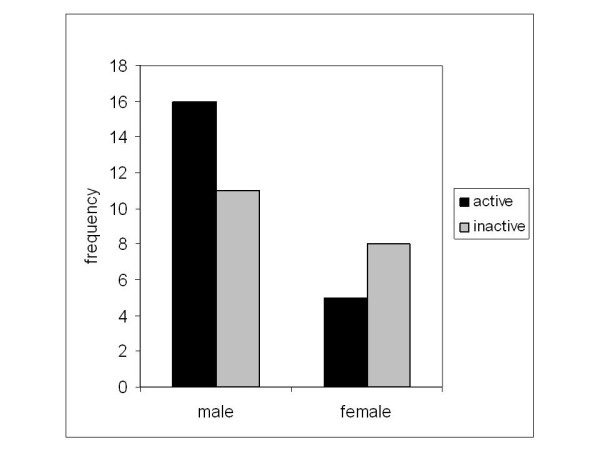
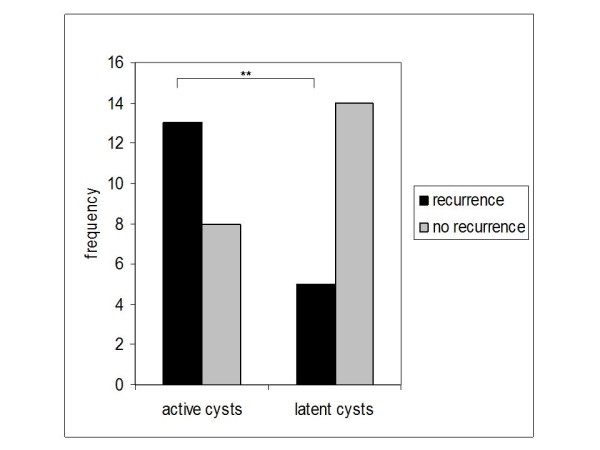
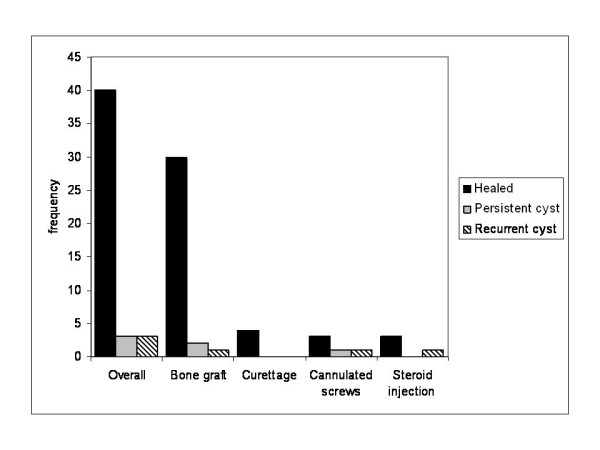
Results: Forty-six patients (17 female, 29 male) with a mean age of 10.0 ± 4.8 years and with histopathologically confirmed diagnosis of UBC were included. Pathological fractures were observed in 21 cases (46%). All patients underwent surgery for UBC (35 patients underwent curettage and bone grafting as a primary therapy, 4 curettage alone, 3 received corticoid instillation and 4 decompression by cannulated screws). Overall recurrence rate after the first surgical treatment was 39% (18/46), second (17.4% of all patients) and third recurrence (4.3%) were frequently observed and were addressed by revision surgery. Recurrence was significantly higher in young and in male patients as well as in active cysts. After a mean of 52 months, 40 out of 46 cysts were considered healed. Prognosis was significantly better when recurrence was observed later than 30 months after therapy. After a mean follow-up of 15.5 ± 6.2 years, 40 patients acknowledged clinically excellent results, while five reported mild and casual pain. Only one patient reported a mild limitation of range of motion.
Conclusions: Our results suggest satisfactory overall long-term outcome for the surgical treatment of UBC, although short-and mid-term observation show a considerable rate of recurrence independent of the surgical technique.
Figures

References
-
- Baker DM. Benign unicameral bone cysts. Clin Orthop. 1970;71:140–151. - PubMed
-
- Boseker EH, Bickel WH, Dahiin DC. A clinicopathologic study of simple unicameral bone cysts. Surg Gynecol Obstet. 1968;127:550–560. - PubMed
-
- Schreuder HW, Conrad EU, Bruckner JD, Howlett AT, Sorensen LS. Treatment of simple bone cysts in children with curettage and cryosurgery. J Pediatr Orthop. 1997;17:814–820. - PubMed
-
- Virchow R. [Über die Bildung von Knochencysten.] Monatsberichte der Königlich Preussischen Akademie der Wissenschaften. 1876. pp. 369–38. - PubMed
-
- Phemister DB, Gordon JE. The etiology of solitary bone cyst. J Am Med Assoc. 1926;87:1429–1433. doi: 10.1001/jama.1926.02680180001001. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
