

Impact of combining intermittent preventive treatment with home management of malaria in children less than 10 years in a rural area of Senegal: a cluster randomized trial
- PMID: 22166001
- PMCID: PMC3286438
- DOI: 10.1186/1475-2875-10-358
Impact of combining intermittent preventive treatment with home management of malaria in children less than 10 years in a rural area of Senegal: a cluster randomized trial
Abstract
Background: Current malaria control strategies recommend (i) early case detection using rapid diagnostic tests (RDT) and treatment with artemisinin combination therapy (ACT), (ii) pre-referral rectal artesunate, (iii) intermittent preventive treatment and (iv) impregnated bed nets. However, these individual malaria control interventions provide only partial protection in most epidemiological situations. Therefore, there is a need to investigate the potential benefits of integrating several malaria interventions to reduce malaria prevalence and morbidity.
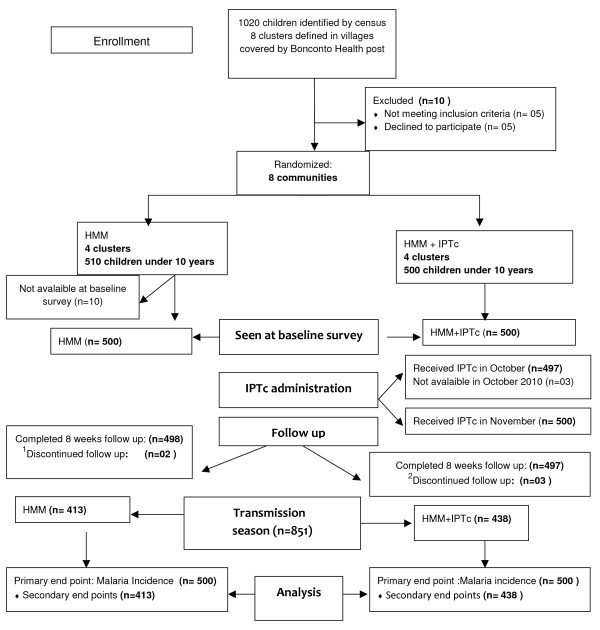
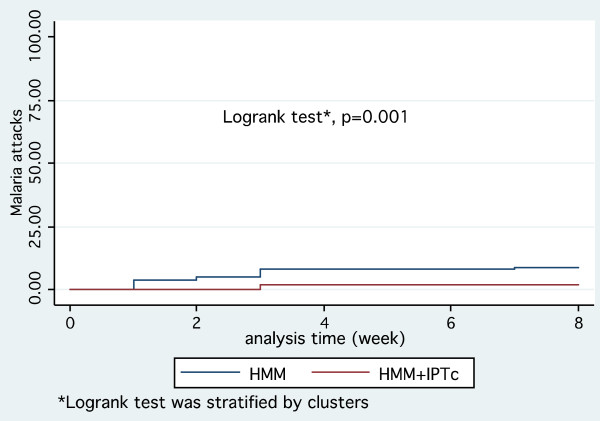
Methods: A randomized controlled trial was carried out to assess the impact of combining seasonal intermittent preventive treatment in children (IPTc) with home-based management of malaria (HMM) by community health workers (CHWs) in Senegal. Eight CHWs in eight villages covered by the Bonconto health post, (South Eastern part of Senegal) were trained to diagnose malaria using RDT, provide prompt treatment with artemether-lumefantrine for uncomplicated malaria cases and pre-referral rectal artesunate for complicated malaria occurring in children under 10 years. Four CHWs were randomized to also administer monthly IPTc as single dose of sulphadoxine-pyrimethamine (SP) plus three doses of amodiaquine (AQ) in the malaria transmission season, October and November 2010. Primary end point was incidence of single episode of malaria attacks over 8 weeks of follow up. Secondary end points included prevalence of malaria parasitaemia, and prevalence of anaemia at the end of the transmission season. Primary analysis was by intention to treat. The study protocol was approved by the Senegalese National Ethical Committee (approval 0027/MSP/DS/CNRS, 18/03/2010).
Results: A total of 1,000 children were enrolled. The incidence of malaria episodes was 7.1/100 child months at risk [95% CI (3.7-13.7)] in communities with IPTc + HMM compared to 35.6/100 child months at risk [95% CI (26.7-47.4)] in communities with only HMM (aOR = 0.20; 95% CI 0.09-0.41; p = 0.04). At the end of the transmission season, malaria parasitaemia prevalence was lower in communities with IPTc + HMM (2.05% versus 4.6% p = 0.03). Adjusted for age groups, sex, Plasmodium falciparum carriage and prevalence of malnutrition, IPTc + HMM showed a significant protective effect against anaemia (aOR = 0.59; 95% CI 0.42-0.82; p = 0.02).
Conclusion: Combining IPTc and HMM can provide significant additional benefit in preventing clinical episodes of malaria as well as anaemia among children in Senegal.
Figures
References
-
- World Health Organization. World malaria report. 2010. ISBN 978 92 4 156410 6 (NLM classification: WC 765)
-
- Adjuik M, Smith T, Clark S, Todd J, Garrib A, Kinfu Y, Kahn K, Mola M, Ashraf A, Masanja H, Adazu K, Sacarlal J, Alam N, Marra A, Gbangou A, Mwageni E, Binka F. Cause-specific mortality rates in sub-Saharan Africa and Bangladesh. Bull World Health Organ. 2006;84:181–188. doi: 10.2471/BLT.05.026492. - DOI - PMC - PubMed
-
- Breman JG, Egan A, Keusch GT. The intolerable burden of malaria: a new look at the numbers. Am J Trop Med Hyg. 2001;64(Suppl 1-2):iv–vii. - PubMed
-
- WHO. Global malaria control and elimination. Technical Consultation Report. Geneva: World Health Organ; 2008. NLM classification: WC 765.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
