

Causes of death among stillbirths
- PMID: 22166605
- PMCID: PMC4562291
- DOI: 10.1001/jama.2011.1823
Causes of death among stillbirths
Abstract
Context: Stillbirth affects 1 in 160 pregnancies in the United States, equal to the number of infant deaths each year. Rates are higher than those of other developed countries and have stagnated over the past decade. There is significant racial disparity in the rate of stillbirth that is unexplained.
Objective: To ascertain the causes of stillbirth in a population that is diverse by race/ethnicity and geography.
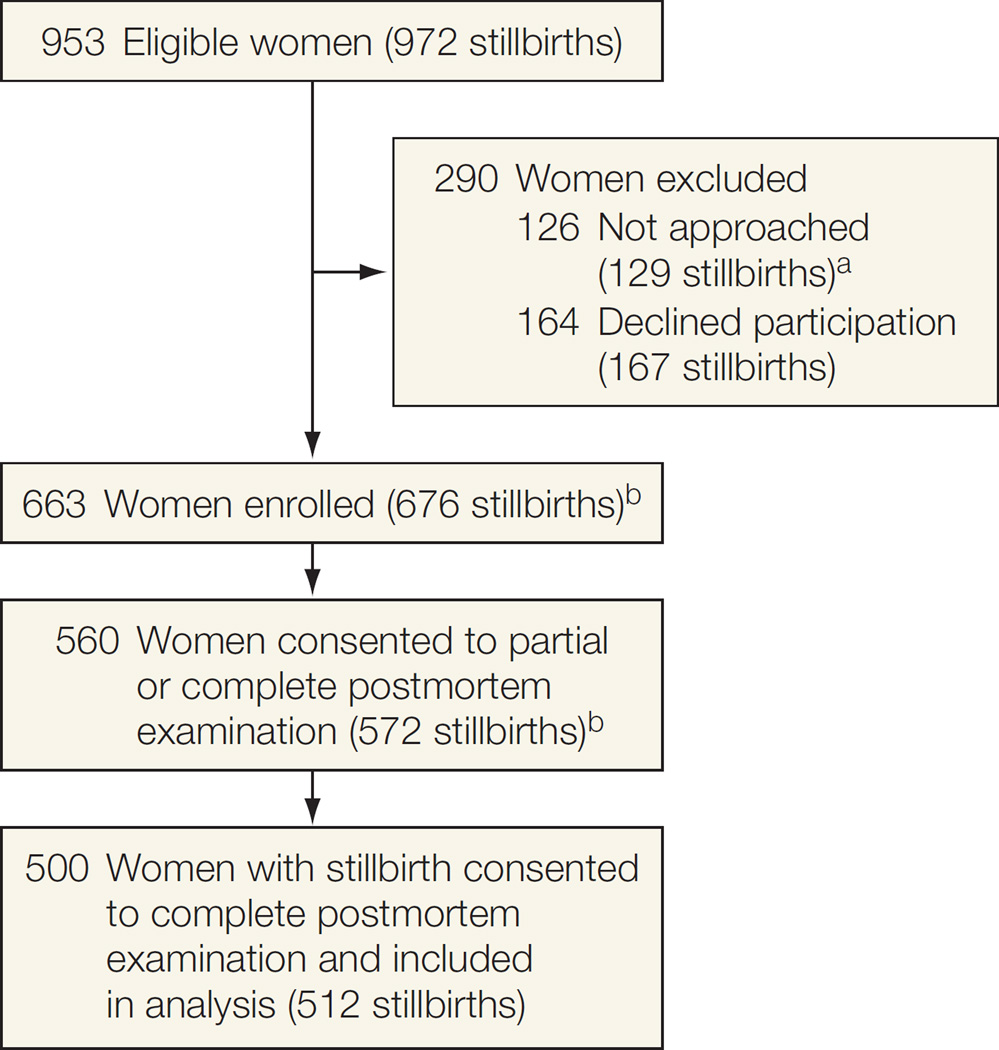
Design, setting, and participants: A population-based study from March 2006 to September 2008 with surveillance for all stillbirths at 20 weeks or later in 59 tertiary care and community hospitals in 5 catchment areas defined by state and county boundaries to ensure access to at least 90% of all deliveries. Termination of a live fetus was excluded. Standardized evaluations were performed at delivery.
Main outcome measures: Medical history, fetal postmortem and placental pathology, karyotype, other laboratory tests, systematic assignment of causes of death.
Results: Of 663 women with stillbirth enrolled, 500 women consented to complete postmortem examinations of 512 neonates. A probable cause of death was found in 312 stillbirths (60.9%; 95% CI, 56.5%-65.2%) and possible or probable cause in 390 (76.2%; 95% CI, 72.2%-79.8%). The most common causes were obstetric conditions (150 [29.3%; 95% CI, 25.4%-33.5%]), placental abnormalities (121 [23.6%; 95% CI, 20.1%-27.6%]), fetal genetic/structural abnormalities (70 [13.7%; 95% CI, 10.9%-17.0%]), infection (66 [12.9%; 95% CI, 10.2%-16.2%]), umbilical cord abnormalities (53 [10.4%; 95% CI, 7.9%-13.4%]), hypertensive disorders (47 [9.2%; 95% CI, 6.9%-12.1%]), and other maternal medical conditions (40 [7.8%; 95% CI, 5.7%-10.6%]). A higher proportion of stillbirths in non-Hispanic black women compared with non-Hispanic white and Hispanic ones was associated with obstetric complications (43.5% [50] vs 23.7% [85]; difference, 19.8%; 95% CI, 9.7%-29.9%; P < .001) and infections (25.2% [29] vs 7.8% [28]; difference, 17.4%; 95% CI, 9.0%-25.8%; P < .001). Stillbirths occurring intrapartum and early in gestation were more common in non-Hispanic black women. Sources most likely to provide positive information regarding cause of death were placental histology (268 [52.3%; 95% CI, 47.9%-56.7%]), perinatal postmortem examination (161 [31.4%; 95% CI, 27.5%-35.7%]), and karyotype (32 of 357 with definitive results [9%; 95% CI, 6.3%-12.5%]).
Conclusions: A systematic evaluation led to a probable or possible cause in the majority of stillbirths. Obstetric conditions and placental abnormalities were the most common causes of stillbirth, although the distribution differed by race/ethnicity.
Conflict of interest statement
Figures
Comment in
-
Stillbirth and lessons for pregnancy care.JAMA. 2011 Dec 14;306(22):2506-7. doi: 10.1001/jama.2011.1822. JAMA. 2011. PMID: 22166612 No abstract available.
References
-
- MacDorman MF, Kirmeyer S. Fetal and perinatal mortality, United States, 2005. Natl Vital Stat Rep. 2009;57(8):1–19. - PubMed
-
- Macdorman MF, Mathews TJ. Recent trends in infant mortality in the United States. NCHS Data Brief. 2008;9(9):1–8. - PubMed
-
- Cousens S, Blencowe H, Stanton C, et al. National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. Lancet. 2011;377(9774):1319–1330. - PubMed
-
- Health Data OECD. [Accessed August 14, 2011];2008 Statistics and indicators for 30 countries. http://www.ecosante.org/index2.php?base=OCDE&langh=ENG&langs=ENG.
-
- Graafmans WC, Richardus JH, Macfarlane A, et al. EuroNatal Working Group. Comparability of published perinatal mortality rates in Western Europe: the quantitative impact of differences in gestational age and birthweight criteria. BJOG. 2001;108(12):1237–1245. - PubMed
