

Intracranial hemorrhage
- PMID: 22167847
- PMCID: PMC3361326
- DOI: 10.1164/rccm.201103-0475CI
Intracranial hemorrhage
Abstract
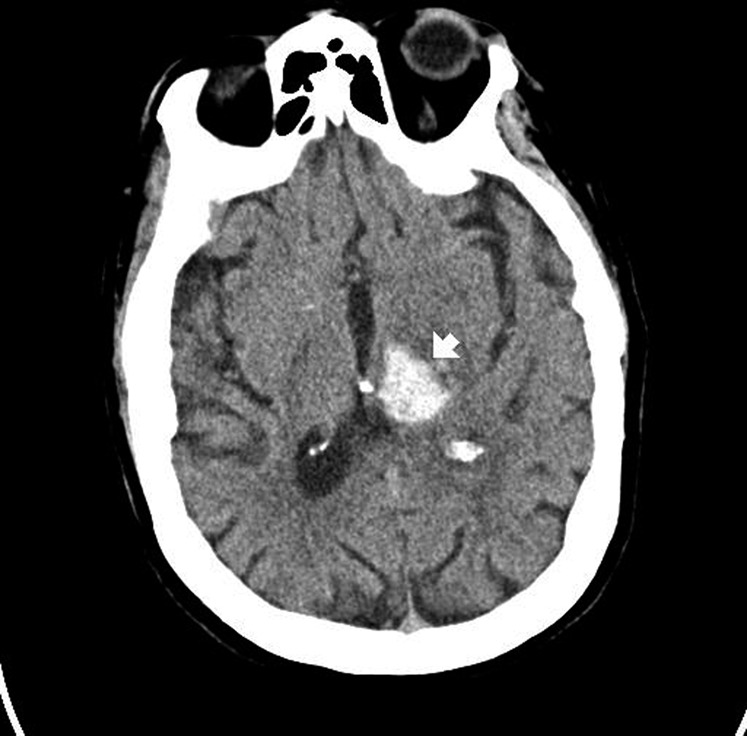
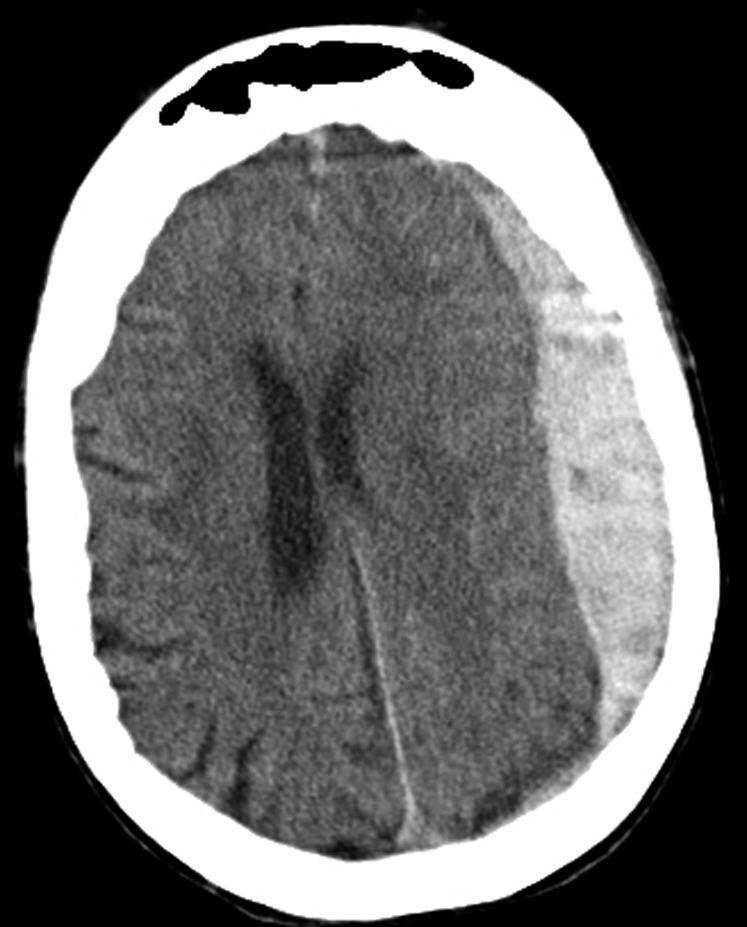
Intracranial hemorrhage is a life-threatening condition, the outcome of which can be improved by intensive care. Intracranial hemorrhage may be spontaneous, precipitated by an underlying vascular malformation, induced by trauma, or related to therapeutic anticoagulation. The goals of critical care are to assess the proximate cause, minimize the risks of hemorrhage expansion through blood pressure control and correction of coagulopathy, and obliterate vascular lesions with a high risk of acute rebleeding. Simple bedside scales and interpretation of computed tomography scans assess the severity of neurological injury. Myocardial stunning and pulmonary edema related to neurological injury should be anticipated, and can usually be managed. Fever (often not from infection) is common and can be effectively treated, although therapeutic cooling has not been shown to improve outcomes after intracranial hemorrhage. Most functional and cognitive recovery takes place weeks to months after discharge; expected levels of functional independence (no disability, disability but independence with a device, dependence) may guide conversations with patient representatives. Goals of care impact mortality, with do-not-resuscitate status increasing the predicted mortality for any level of severity of intraparenchymal hemorrhage. Future directions include refining the use of bedside neuro-monitoring (electroencephalogram, invasive monitors), novel approaches to reduce intracranial hemorrhage expansion, minimizing vasospasm, and refining the assessment of quality of life to guide rehabilitation and therapy.
Figures

References
-
- Delgado Almandoz JE, Yoo AJ, Stone MJ, Schaefer PW, Goldstein JN, Rosand J, Oleinik A, Lev MH, Gonzalez RG, Romero JM. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke 2009;40:2994–3000 - PMC - PubMed
-
- Mayer SA, Bernardini GL, Solomon RA. Subarachnoid hemorrhage. In: Rowland LP, Pedley TA, editors Merritt's neurology, 12th ed Philadelphia: Lippincott Williams & Wilkins; 2010
-
- van der Schaaf IC, Velthuis BK, Gouw A, Rinkel GJE. Venous drainage in perimesencephalic hemorrhage. Stroke 2004;35:1614–1618 - PubMed
-
- He J, Whelton PK, Vu B, Klag M. Aspirin and the risk of hemorrhage stroke: a meta-analysis of randomized controlled trials. JAMA 1998;280:1930–1935 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
