

Liberal or restrictive transfusion in high-risk patients after hip surgery
- PMID: 22168590
- PMCID: PMC3268062
- DOI: 10.1056/NEJMoa1012452
Liberal or restrictive transfusion in high-risk patients after hip surgery
Abstract
Background: The hemoglobin threshold at which postoperative red-cell transfusion is warranted is controversial. We conducted a randomized trial to determine whether a higher threshold for blood transfusion would improve recovery in patients who had undergone surgery for hip fracture.
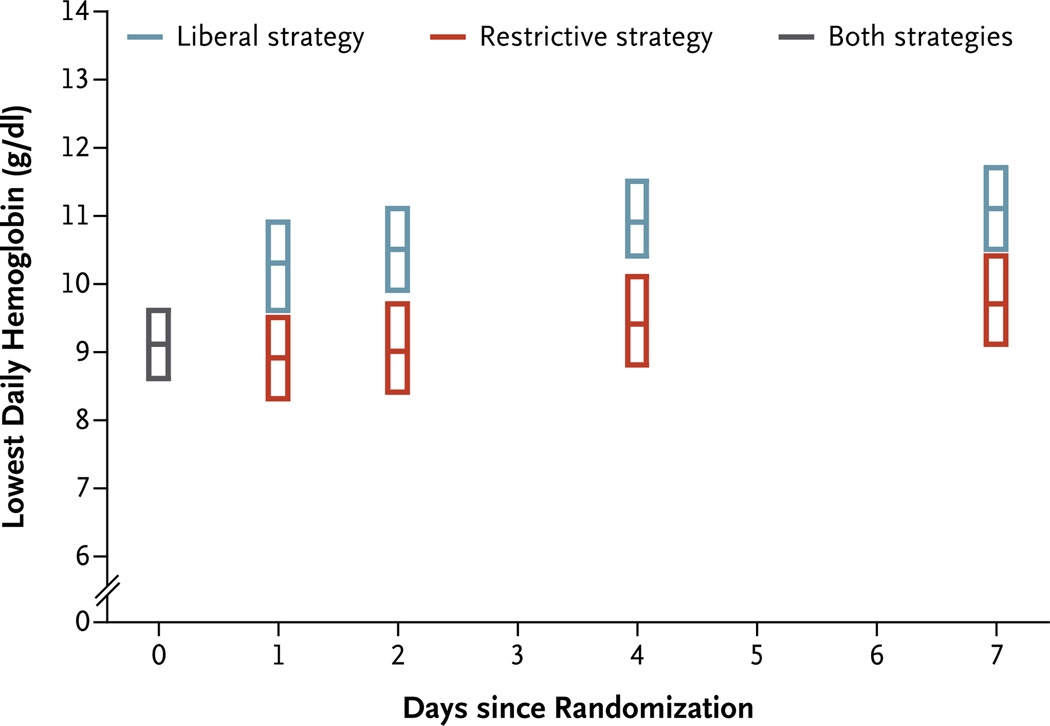
Methods: We enrolled 2016 patients who were 50 years of age or older, who had either a history of or risk factors for cardiovascular disease, and whose hemoglobin level was below 10 g per deciliter after hip-fracture surgery. We randomly assigned patients to a liberal transfusion strategy (a hemoglobin threshold of 10 g per deciliter) or a restrictive transfusion strategy (symptoms of anemia or at physician discretion for a hemoglobin level of <8 g per deciliter). The primary outcome was death or an inability to walk across a room without human assistance on 60-day follow-up.
Results: A median of 2 units of red cells were transfused in the liberal-strategy group and none in the restrictive-strategy group. The rates of the primary outcome were 35.2% in the liberal-strategy group and 34.7% in the restrictive-strategy group (odds ratio in the liberal-strategy group, 1.01; 95% confidence interval [CI], 0.84 to 1.22), for an absolute risk difference of 0.5 percentage points (95% CI, -3.7 to 4.7). The rates of in-hospital acute coronary syndrome or death were 4.3% and 5.2%, respectively (absolute risk difference, -0.9%; 99% CI, -3.3 to 1.6), and rates of death on 60-day follow-up were 7.6% and 6.6%, respectively (absolute risk difference, 1.0%; 99% CI, -1.9 to 4.0). The rates of other complications were similar in the two groups.
Conclusions: A liberal transfusion strategy, as compared with a restrictive strategy, did not reduce rates of death or inability to walk independently on 60-day follow-up or reduce in-hospital morbidity in elderly patients at high cardiovascular risk. (Funded by the National Heart, Lung, and Blood Institute; FOCUS ClinicalTrials.gov number, NCT00071032.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Transfusion thresholds in FOCUS.N Engl J Med. 2011 Dec 29;365(26):2532-3. doi: 10.1056/NEJMe1110087. Epub 2011 Dec 14. N Engl J Med. 2011. PMID: 22168589 No abstract available.
-
Transfusion thresholds in high-risk patients after hip surgery.N Engl J Med. 2012 Mar 29;366(13):1253; author reply 1254-5. doi: 10.1056/NEJMc1201459. N Engl J Med. 2012. PMID: 22455422 No abstract available.
-
Transfusion thresholds in high-risk patients after hip surgery.N Engl J Med. 2012 Mar 29;366(13):1253-4; author reply 1254-5. doi: 10.1056/NEJMc1201459. N Engl J Med. 2012. PMID: 22455423 No abstract available.
-
Transfusion thresholds in high-risk patients after hip surgery.N Engl J Med. 2012 Mar 29;366(13):1254; author reply 1254-5. doi: 10.1056/NEJMc1201459. N Engl J Med. 2012. PMID: 22455424 No abstract available.
-
[Hip fractures - transfusion management after hip surgery].Z Orthop Unfall. 2012 Apr;150(2):134. Z Orthop Unfall. 2012. PMID: 22611557 German. No abstract available.
References
-
- Washington, DC: Department of Health and Human Services, Office of the Assistant Secretary for Health; 2011. Report of the Department of Health and Human Services: the 2009 national blood collection and utilization survey report.
-
- Anderson SA, Menis M, O’Connell K, Burwen DR. Blood use by inpatient elderly population in the United States. Transfusion. 2007;47:582–592. - PubMed
-
- Cobain TJ, Vamvakas EC, Wells A, Titlestad K. A survey of the demographics of blood use. Transfus Med. 2007;17:1–15. - PubMed
-
- Carless PA, Henry DA, Carson JL, Hebert PP, McClelland B, Ker K. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2010;10 CD002042. - PubMed
-
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409–417. [Erratum, N Engl J Med 1999;340:1056.] - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical