

Cardiovascular magnetic resonance tagging of the right ventricular free wall for the assessment of long axis myocardial function in congenital heart disease
- PMID: 22168638
- PMCID: PMC3286381
- DOI: 10.1186/1532-429X-13-80
Cardiovascular magnetic resonance tagging of the right ventricular free wall for the assessment of long axis myocardial function in congenital heart disease
Abstract
Background: Right ventricular ejection fraction (RV-EF) has traditionally been used to measure and compare RV function serially over time, but may be a relatively insensitive marker of change in RV myocardial contractile function. We developed a cardiovascular magnetic resonance (CMR) tagging-based technique with a view to rapid and reproducible measurement of RV long axis function and applied it in patients with congenital heart disease.
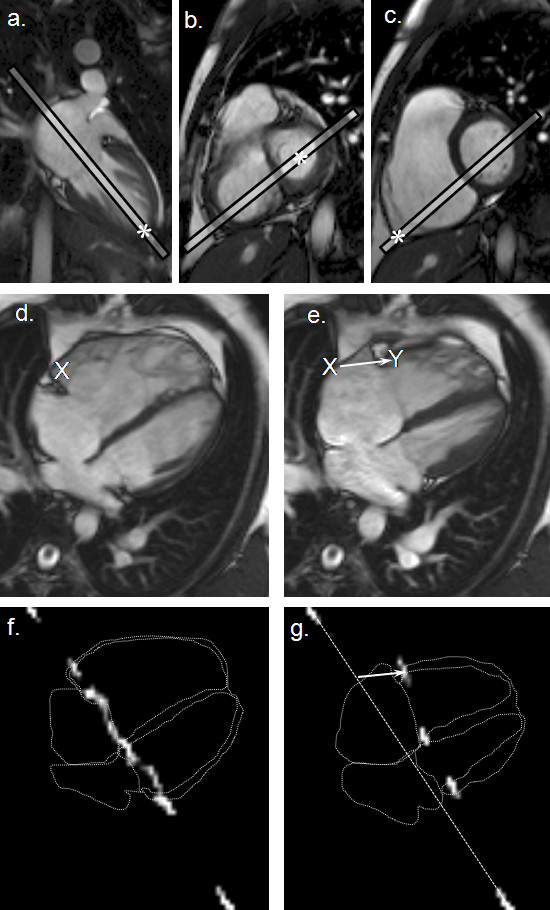
Methods: We studied 84 patients: 56 with repaired Tetralogy of Fallot (rTOF); 28 with atrial septal defect (ASD): 13 with and 15 without pulmonary hypertension (RV pressure > 40 mmHG by echocardiography). For comparison, 20 healthy controls were studied. CMR acquisitions included an anatomically defined four chamber cine followed by a cine gradient echo-planar sequence in the same plane with a labelling pre-pulse giving a tag line across the basal myocardium. RV tag displacement was measured with automated registration and tracking of the tag line together with standard measurement of RV-EF.
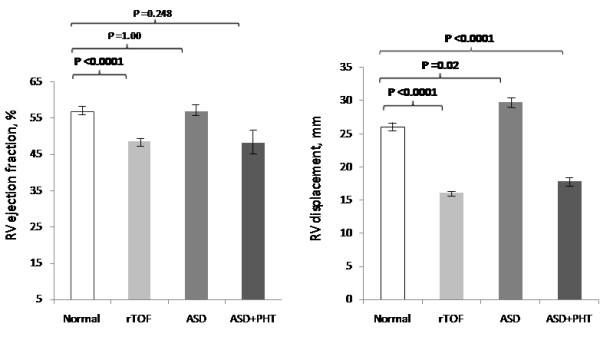
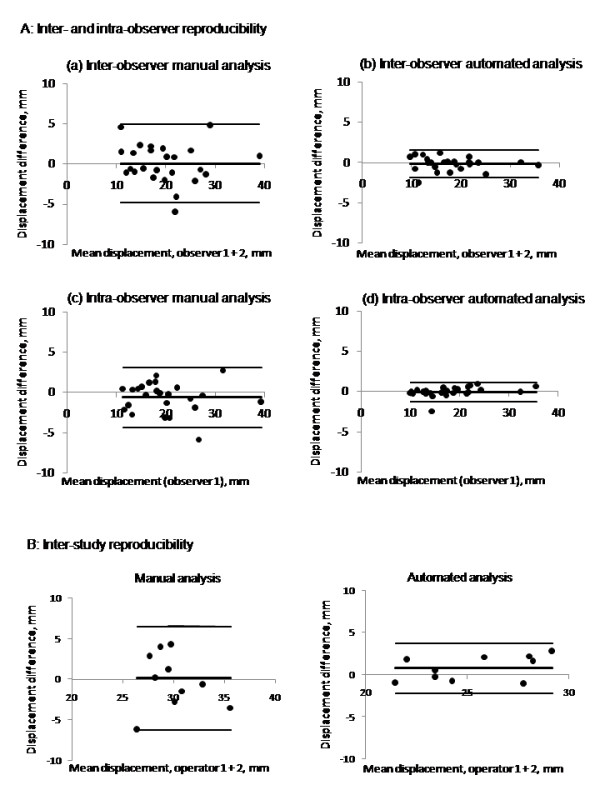
Results: Mean RV displacement was higher in the control (26 ± 3 mm) than in rTOF (16 ± 4 mm) and ASD with pulmonary hypertension (18 ± 3 mm) groups, but lower than in the ASD group without (30 ± 4 mm), P < 0.001. The technique was reproducible with inter-study bias ± 95% limits of agreement of 0.7 ± 2.7 mm. While RV-EF was lower in rTOF than in controls (49 ± 9% versus 57 ± 6%, P < 0.001), it did not differ between either ASD group and controls.
Conclusions: Measurements of RV long axis displacement by CMR tagging showed more differences between the groups studied than did RV-EF, and was reproducible, quick and easy to apply. Further work is needed to assess its potential use for the detection of longitudinal changes in RV myocardial function.
© 2011 Chen et al; licensee BioMed Central Ltd.
Figures
References
-
- Naito H, Arisawa J, Harada K, Yamagami H, Kozuka T, Tamura S. Assessment of right ventricular regional contraction and comparison with the left ventricle in normal humans: a cine magnetic resonance study with presaturation myocardial tagging. Br Heart J. 1995;74:186–191. doi: 10.1136/hrt.74.2.186. - DOI - PMC - PubMed
