

Pathogens and the placental fortress
- PMID: 22169833
- PMCID: PMC3265690
- DOI: 10.1016/j.mib.2011.11.006
Pathogens and the placental fortress
Abstract
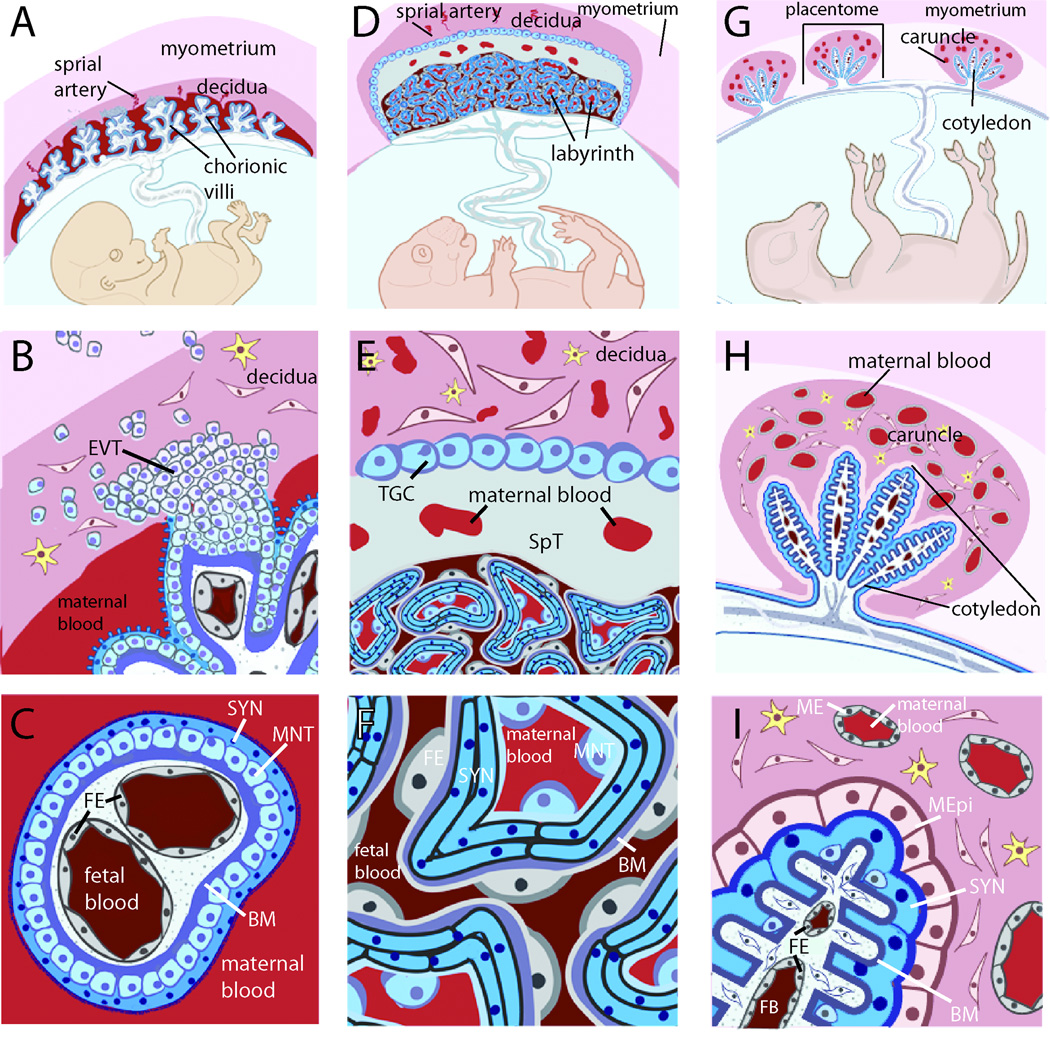
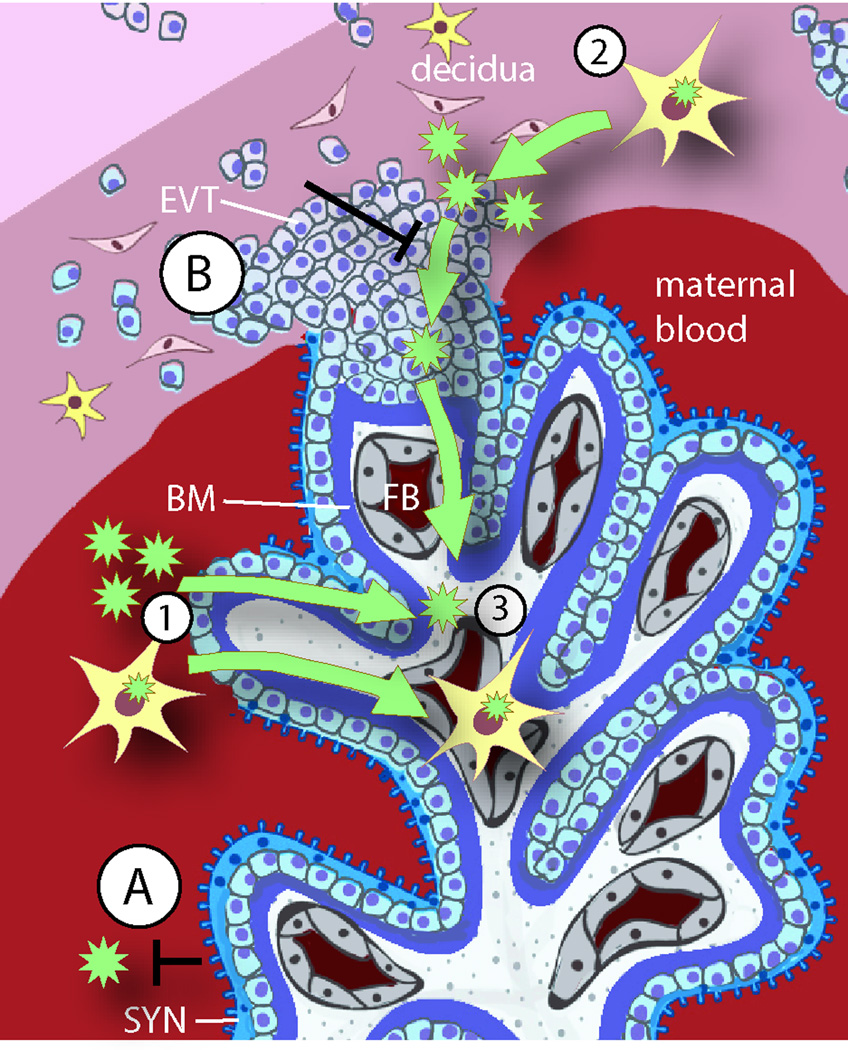
Placental infections are major causes of maternal and fetal disease. This review introduces a new paradigm for placental infections based on current knowledge of placental defenses and how this barrier can be breached. Transmission of pathogens from mother to fetus can occur at two sites of direct contact between maternal cells and specialized fetal cells (trophoblasts) in the human placenta: firstly, maternal immune and endothelial cells juxtaposed to extravillous trophoblasts in the uterine implantation site and secondly, maternal blood surrounding the syncytiotrophoblast (SYN). Recent findings suggest that the primary vulnerability is in the implantation site. We explore evidence that the placental SYN evolved as a defense against pathogens, and that inflammation-mediated spontaneous abortion may benefit mother and pathogen.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371(9608):261–269. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
