

The role of neuronavigation in intracranial endoscopic procedures
- PMID: 22170178
- PMCID: PMC3375008
- DOI: 10.1007/s10143-011-0369-7
The role of neuronavigation in intracranial endoscopic procedures
Abstract
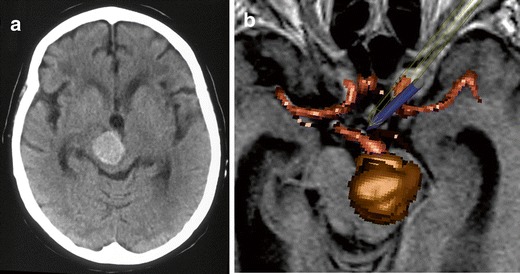
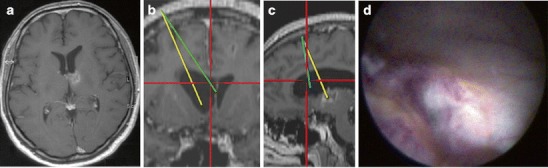
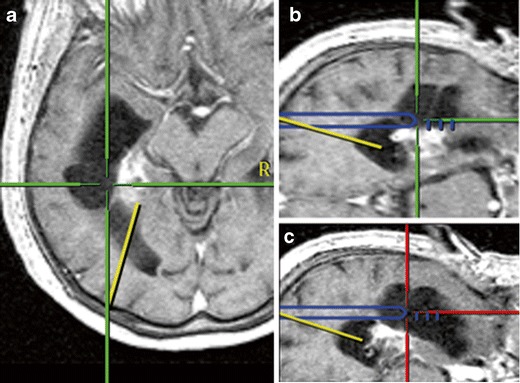
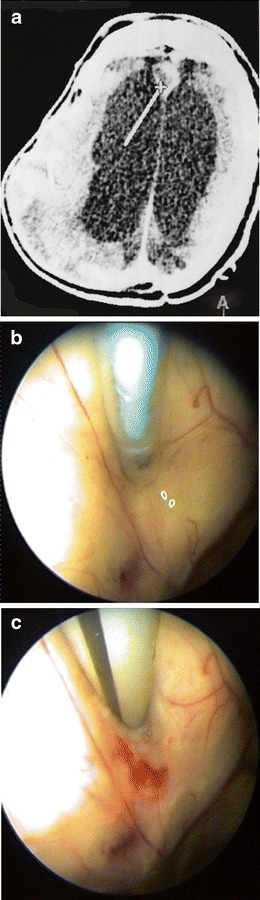
In occlusive hydrocephalus, cysts and some ventricular tumours, neuroendoscopy has replaced shunt operations and microsurgery. There is an ongoing discussion if neuronavigation should routinely accompany neuroendoscopy or if its use should be limited to selected cases. In this prospective clinical series, the role of neuronavigation during intracranial endoscopic procedures was investigated. In 126 consecutive endoscopic procedures (endoscopic third ventriculostomy, ETV, n = 65; tumour biopsy/resection, n = 36; non-tumourous cyst fenestration, n = 23; abscess aspiration and hematoma removal, n = 1 each), performed in 121 patients, neuronavigation was made available. After operation and videotape review, the surgeon had to categorize the role of neuronavigation: not beneficial; beneficial, but not essential; essential. Overall, neuronavigation was of value in more than 50% of the operations, but its value depended on the type of the procedure. Neuronavigation was beneficial, but not essential in 16 ETVs (24.6%), 19 tumour biopsies/resections (52.7%) and 14 cyst fenestrations (60.9%). Neuronavigation was essential in 1 ETV (2%), 11 tumour biopsies/resections (30.6%) and 8 cyst fenestrations (34.8%). Neuronavigation was not needed/not used in 48 ETVs (73.9%), 6 endoscopic tumour operations (16.7%) and 1 cyst fenestration (4.3%). For ETV, neuronavigation mostly is not required. In the majority of the remaining endoscopic procedures, however, neuronavigation is at least beneficial. This finding suggests integrating neuronavigation into the operative routine in endoscopic tumour operations and cyst fenestrations.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
