

Quantification of increased cellularity during inflammatory demyelination
- PMID: 22171354
- PMCID: PMC3235568
- DOI: 10.1093/brain/awr307
Quantification of increased cellularity during inflammatory demyelination
Abstract
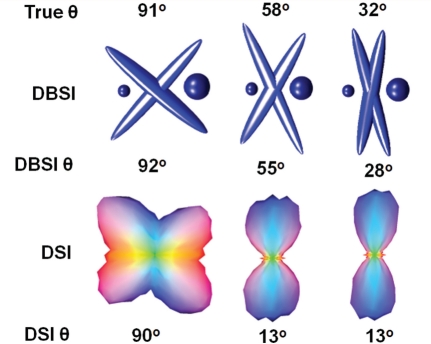
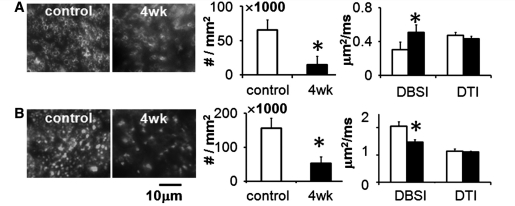
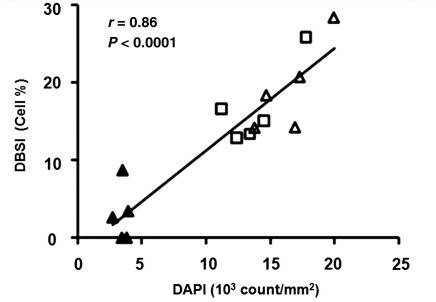
Multiple sclerosis is characterized by inflammatory demyelination and irreversible axonal injury leading to permanent neurological disabilities. Diffusion tensor imaging demonstrates an improved capability over standard magnetic resonance imaging to differentiate axon from myelin pathologies. However, the increased cellularity and vasogenic oedema associated with inflammation cannot be detected or separated from axon/myelin injury by diffusion tensor imaging, limiting its clinical applications. A novel diffusion basis spectrum imaging, capable of characterizing water diffusion properties associated with axon/myelin injury and inflammation, was developed to quantitatively reveal white matter pathologies in central nervous system disorders. Tissue phantoms made of normal fixed mouse trigeminal nerves juxtaposed with and without gel were employed to demonstrate the feasibility of diffusion basis spectrum imaging to quantify baseline cellularity in the absence and presence of vasogenic oedema. Following the phantom studies, in vivo diffusion basis spectrum imaging and diffusion tensor imaging with immunohistochemistry validation were performed on the corpus callosum of cuprizone treated mice. Results demonstrate that in vivo diffusion basis spectrum imaging can effectively separate the confounding effects of increased cellularity and/or grey matter contamination, allowing successful detection of immunohistochemistry confirmed axonal injury and/or demyelination in middle and rostral corpus callosum that were missed by diffusion tensor imaging. In addition, diffusion basis spectrum imaging-derived cellularity strongly correlated with numbers of cell nuclei determined using immunohistochemistry. Our findings suggest that diffusion basis spectrum imaging has great potential to provide non-invasive biomarkers for neuroinflammation, axonal injury and demyelination coexisting in multiple sclerosis.
Figures




References
-
- Alexander DC. Multiple-fiber reconstruction algorithms for diffusion MRI. Ann N Y Acad Sci. 2005;1064:113–33. - PubMed
-
- Alexander DC, Hubbard PL, Hall MG, Moore EA, Ptito M, Parker GJ, et al. Orientationally invariant indices of axon diameter and density from diffusion MRI. Neuroimage. 2010;52:1374–89. - PubMed
-
- Anderson AW. Measurement of fiber orientation distributions using high angular resolution diffusion imaging. Magn Reson Med. 2005;54:1194–206. - PubMed
-
- Anderson AW, Xie J, Pizzonia J, Bronen RA, Spencer DD, Gore JC. Effects of cell volume fraction changes on apparent diffusion in human cells. Magn Reson Imaging. 2000;18:689–95. - PubMed
-
- Audet C, Dennis JE. Analysis of generalized pattern searches. Siam J Optimization. 2003;13:889–903.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
