

Long term incidence of dementia, predictors of mortality and pathological diagnosis in older stroke survivors
- PMID: 22171356
- PMCID: PMC3235558
- DOI: 10.1093/brain/awr273
Long term incidence of dementia, predictors of mortality and pathological diagnosis in older stroke survivors
Abstract
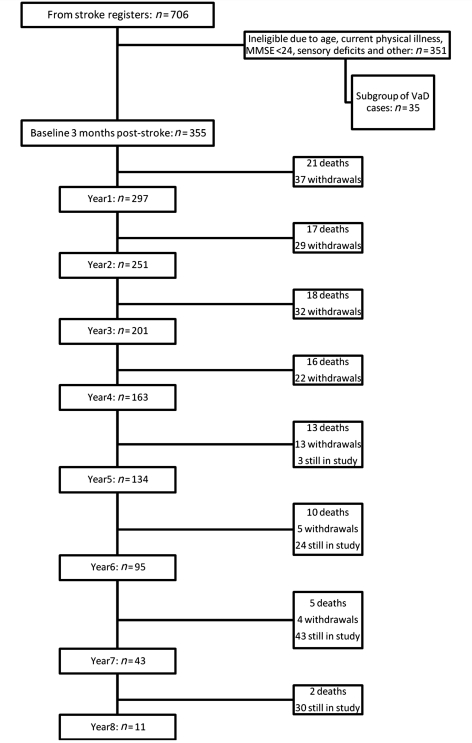
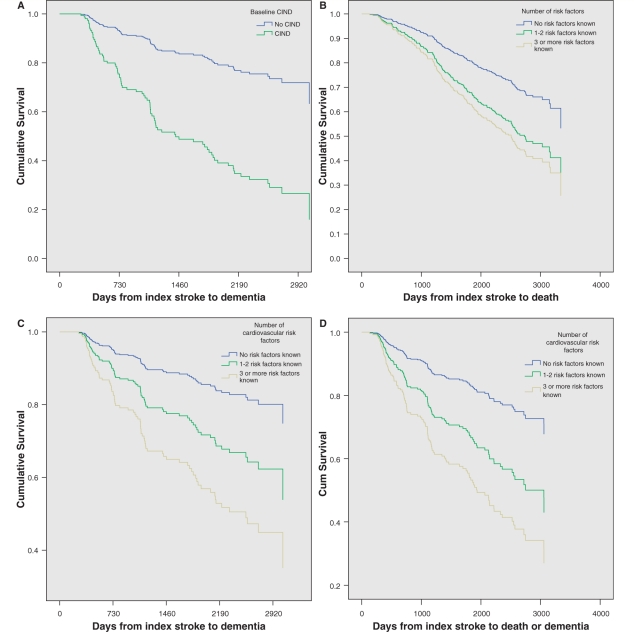
Greater understanding of the risk factors and mechanisms of incident dementia in stroke survivors is needed for prevention and management. There is limited information on the long-term consequences and forms of incident dementia in older stroke survivors. We recruited 355 patients aged >75 years from hospital-based stroke registers into a longitudinal study 3 months after stroke. At baseline none of the patients had dementia. Patients were genotyped for apolipoprotein E and assessed annually for cognition and development of incident dementia over up to 8 years of follow-up. The effect of baseline vascular risk factors upon incidence of dementia and mortality were estimated by Cox proportional regression analyses adjusted for age and gender. Standard neuropathological examination was performed to diagnose the first 50 cases that came to autopsy. We found that the median survival from the date of the index stroke was 6.72 years (95% confidence intervals: 6.38-7.05). During the follow-up of a mean time of 3.79 years, 23.9% of subjects were known to have developed dementia and 76.1% remained alive without dementia or died without dementia. The incidence of delayed dementia was calculated to be 6.32 cases per 100 person years whereas that for death or dementia was 8.62. Univariate and multivariate regression analyses showed that the most robust predictors of dementia included low (1.5 standard deviations below age-matched control group) baseline Cambridge Cognitive Examination executive function and memory scores, Geriatric Depression Scale score and three or more cardiovascular risk factors. Autopsy findings suggested that remarkably ≥ 75% of the demented stroke survivors met the current criteria for vascular dementia. Demented subjects tended to exhibit marginally greater neurofibrillary pathology including tauopathy and Lewy bodies and microinfarcts than non-demented survivors. Despite initial improvements in cognition following stroke in older stroke survivors, risk of progression to delayed dementia after stroke is substantial, but is related to the presence of vascular risk factors. Careful monitoring and treatment of modifiable vascular risk factors may be of benefit in preventing post-stroke dementia in the general population.
Figures
References
-
- Altieri M, Di Piero V, Pasquini M, Gasparini M, Vanacore N, Vicenzini E, et al. Delayed poststroke dementia: a 4-year follow-up study. Neurology. 2004;62:2193–7. - PubMed
-
- Ballard C, Rowan E, Stephens S, Kalaria R, Kenny RA. Prospective follow-up study between 3 and 15 months after stroke: improvements and decline in cognitive function among dementia-free stroke survivors >75 years of age. Stroke. 2003a;34:2440–4. - PubMed
-
- Ballard C, Stephens S, Kenny R, Kalaria R, Tovee M, O'Brien J. Profile of neuropsychological deficits in older stroke survivors without dementia. Dement Geriatr Cogn Disord. 2003b;16:52–6. - PubMed
-
- Ballard CG, Morris CM, Rao H, O'Brien JT, Barber R, Stephens S, et al. APOE epsilon4 and cognitive decline in older stroke patients with early cognitive impairment. Neurology. 2004;63:1399–402. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
