

Research priorities in surgical simulation for the 21st century
- PMID: 22172482
- PMCID: PMC3322506
- DOI: 10.1016/j.amjsurg.2011.05.008
Research priorities in surgical simulation for the 21st century
Abstract
Background: Despite tremendous growth, research in surgical simulation remains uncoordinated and unfocused. The objective of this study was to develop research priorities for surgical simulation.
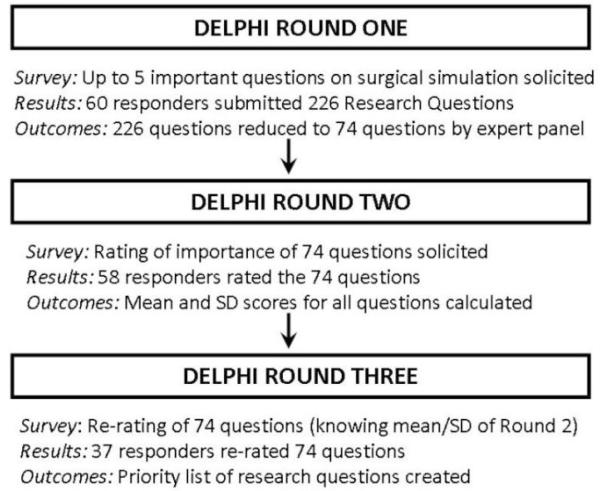
Methods: By using a systematic methodology (Delphi), members of the Association for Surgical Education submitted 5 research questions on surgical simulation. An expert review panel categorized and collapsed the submitted questions and redistributed them to the membership to be ranked using a priority scale from 1 (lowest) to 5 (highest). The results were analyzed and categorized by consensus in distinct topics.
Results: Sixty members submitted 226 research questions that were reduced to 74. Ratings ranged from 2.19 to 4.78. Topics included simulation effectiveness and outcomes, performance assessment and credentialing, curriculum development, team training and nontechnical skills, simulation center resources and personnel, simulator validation, and other. The highest ranked question was, "Does simulation training lead to improved quality of patient care, patient outcomes, and safety?".
Conclusions: Research priorities for surgical simulation were developed using a systematic methodology and can be used to focus surgical simulation research in areas most likely to advance the field.
Copyright © 2012 Elsevier Inc. All rights reserved.
References
-
- Ahlberg G, Enochsson L, Gallagher AG, et al. Proficiency-based virtual reality training significantly reduces the error rate for residents during their first 10 laparoscopic cholecystectomies. Am J Surg. 2007;193:797–804. - PubMed
-
- Scott DJ, Bergen PC, Rege RV, et al. Laparoscopic training on bench models: better and more cost effective than operating room experience? J Am Coll Surg. 2000;191:272–83. - PubMed
-
- Scott DJ, Dunnington GL. The New ACS/APDS Skills Curriculum: Moving the Learning Curve Out of the Operating Room. J Gastrointest Surg. 2008;12:213–21. - PubMed
-
- Sachdeva AK, Pellegrini CA, Johnson KA. Support for simulation-based surgical education through American College of Surgeons--accredited education institutes. World J Surg. 2008;32:196–207. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
