

Moderators and mediators of remission in family-based treatment and adolescent focused therapy for anorexia nervosa
- PMID: 22172564
- PMCID: PMC3260378
- DOI: 10.1016/j.brat.2011.11.003
Moderators and mediators of remission in family-based treatment and adolescent focused therapy for anorexia nervosa
Abstract
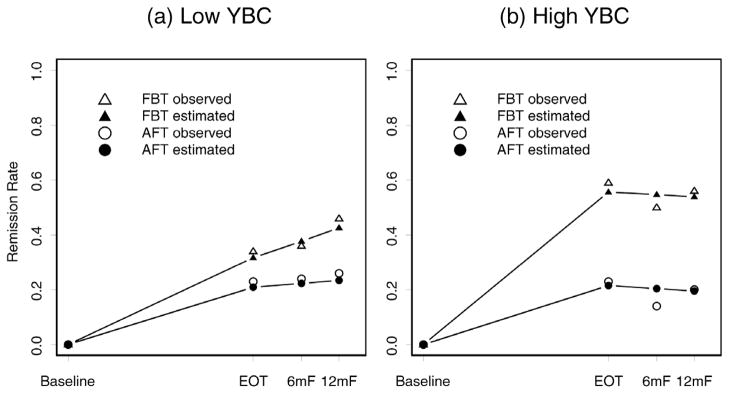
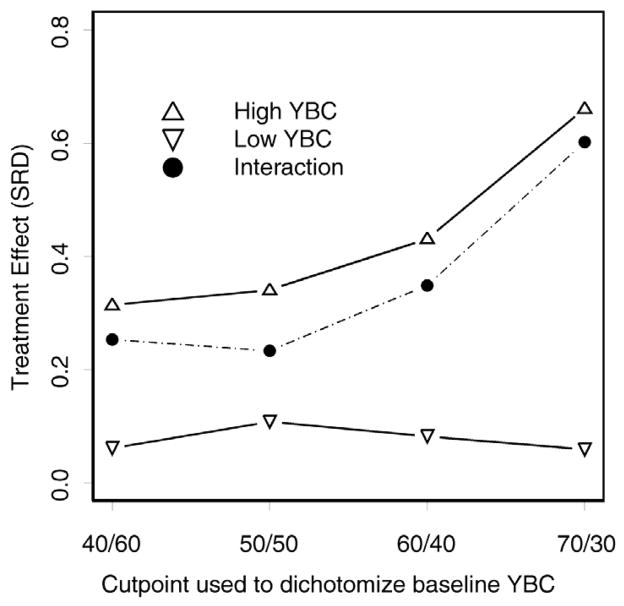
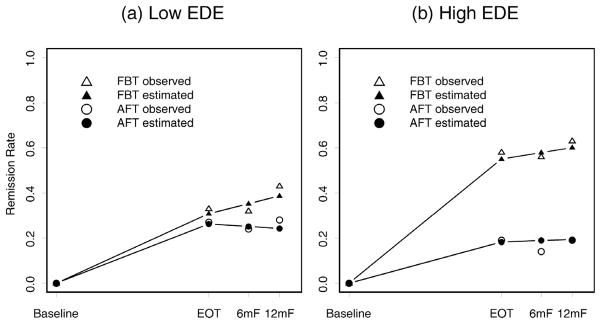
Few of the limited randomized controlled trails (RCTs) for adolescent anorexia nervosa (AN) have explored the effects of moderators and mediators on outcome. This study aimed to identify treatment moderators and mediators of remission at end of treatment (EOT) and 6- and 12-month follow-up (FU) for adolescents with AN (N = 121) who participated in a multi-center RCT of family-based treatment (FBT) and individual adolescent focused therapy (AFT). Mixed effects modeling were utilized and included all available outcome data at all time points. Remission was defined as ≥ 95% IBW plus within 1 SD of the Eating Disorder Examination (EDE) norms. Eating related obsessionality (Yale-Brown-Cornell Eating Disorder Total Scale) and eating disorder specific psychopathology (EDE-Global) emerged as moderators at EOT. Subjects with higher baseline scores on these measures benefited more from FBT than AFT. AN type emerged as a moderator at FU with binge-eating/purging type responding less well than restricting type. No mediators of treatment outcome were identified. Prior hospitalization, older age and duration of illness were identified as non-specific predictors of outcome. Taken together, these results indicate that patients with more severe eating related psychopathology have better outcomes in a behaviorally targeted family treatment (FBT) than an individually focused approach (AFT).
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Agras WS, Crow SJ, Halmi KA, Mitchell JE, Wilson GT, Kraemer HC. Outcome predictors for the cognitive behavior treatment of bulimia nervosa: data from a multisite study. American Journal of Psychiatry. 2000;157:1302–1308. - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington: American Psychiatric Association Press; 2000. Text Revision.
-
- Beck A, Steer R, Brown G. Manual for the Beck Depression Inventory-II. Psychological Corporation; 1996.
-
- Bravender T, Bryant-Waugh R, Herzog D, et al. Classification of child and adolescent eating disturbances. Workgroup for Classification of Eating Disorders in Children and Adolescents (WCEDCA) International Journal of Eating Disorders. 2007;40:S117–S22. - PubMed
-
- Center for Disease Control and Prevention. CDC Growth Charts for the United States: Development and Methods. Atlanta: Center for Disease Control; 2002.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
