

AIDS and non-AIDS morbidity and mortality across the spectrum of CD4 cell counts in HIV-infected adults before starting antiretroviral therapy in Cote d'Ivoire
- PMID: 22173233
- PMCID: PMC3275759
- DOI: 10.1093/cid/cir898
AIDS and non-AIDS morbidity and mortality across the spectrum of CD4 cell counts in HIV-infected adults before starting antiretroviral therapy in Cote d'Ivoire
Abstract
Background: In Western Europe, North America, and Australia, large cohort collaborations have been able to estimate the short-term CD4 cell count-specific risk of AIDS or death in untreated human immunodeficiency virus (HIV)-infected adults with high CD4 cell counts. In sub-Saharan Africa, these CD4 cell count-specific estimates are scarce.
Methods: From 1996 through 2006, we followed up 2 research cohorts of HIV-infected adults in Côte d'Ivoire. This included follow-up off antiretroviral therapy (ART) across the entire spectrum of CD4 cell counts before the ART era, and only in patients with CD4 cell counts >200 cells/μL once ART became available. Data were censored at ART initiation. We modeled the CD4 cell count decrease using an adjusted linear mixed model. CD4 cell count-specific rates of events were obtained by dividing the number of first events occurring in a given CD4 cell count stratum by the time spent in that stratum.
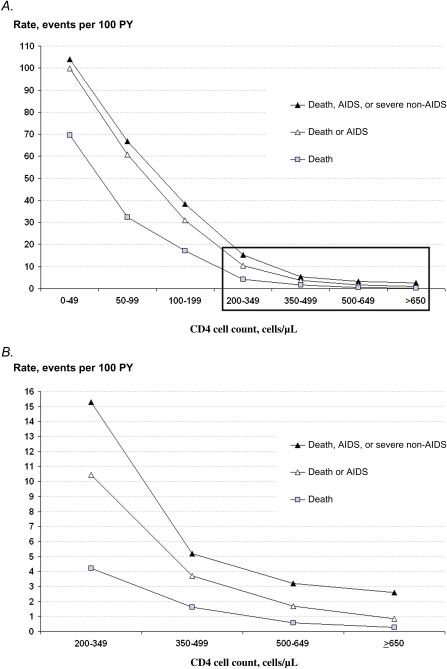
Results: Eight hundred sixty patients were followed off ART over 2789 person-years (PY). In the ≥650, 500-649, 350-499, 200-349, 100-199, 50-99, and 0-49 cells/μL CD4 cell count strata, the rates of AIDS or death were 0.9, 1.7, 3.7, 10.4, 30.9, 60.8, and 99.9 events per 100 PY, respectively. In patients with CD4 cell counts ≥200 CD4 cells/μL, the most frequent AIDS-defining disease was tuberculosis (decreasing from 4.0 to 0.6 events per 100 PY for 200-349 and ≥650 cells/μL, respectively), and the most frequent HIV non-AIDS severe diseases were visceral bacterial diseases (decreasing from 9.1 to 3.6 events per 100 PY).
Conclusions: Rates of AIDS or death, tuberculosis, and invasive bacterial diseases are substantial in patients with CD4 cell counts ≥200 cells/μL. Tuberculosis and bacterial diseases should be the most important outcomes in future trials of early ART in sub-Saharan Africa.
Figures
References
-
- Phillips A, Pezzotti P. Short-term risk of AIDS according to current CD4 cell count and viral load in antiretroviral drug–naive individuals and those treated in the monotherapy era. AIDS. 2004;18:51–8. - PubMed
-
- Phillips AN, Gazzard B, Gilson R, et al. Rate of AIDS diseases or death in HIV-infected antiretroviral therapy–naive individuals with high CD4 cell count. AIDS. 2007;21:1717–21. - PubMed
-
- van Oosterhout JJ, Laufer MK, Graham SM, et al. A community-based study of the incidence of trimethoprim-sulfamethoxazole-preventable infections in Malawian adults living with HIV. J Acquir Immune Defic Syndr. 2005;39:626–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
