

Comparative evaluation of 18F-FDOPA, 13N-AMMONIA, 18F-FDG PET/CT and MRI in primary brain tumors - A pilot study
- PMID: 22174511
- PMCID: PMC3237222
- DOI: 10.4103/0972-3919.90256
Comparative evaluation of 18F-FDOPA, 13N-AMMONIA, 18F-FDG PET/CT and MRI in primary brain tumors - A pilot study
Abstract
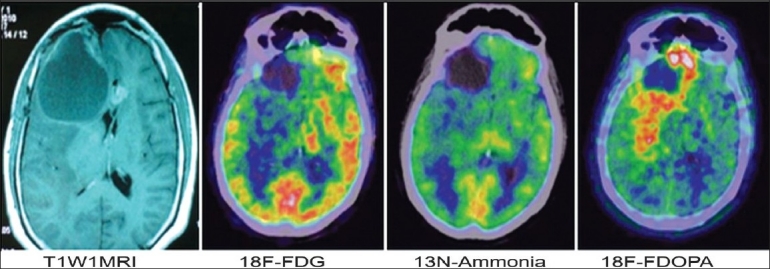
Aim: To determine the diagnostic reliability of 18F-FDOPA, 13N-Ammonia and 18F-FDG PET/CT in primary brain tumors and comparison with magnetic resonance imaging (MRI).
Materials and methods: A total of 23 patients, 8 preoperative and 15 postoperative, undergoing evaluation for primary brain tumors were included in this study. Of them, 9/15 were operated for high grade gliomas (7/9 astrocytomas and 2/9 oligodendrogliomas) and 6/15 for low grade gliomas (5/6 astrocytomas and 1/6 oligodendroglioma). After PET study, 2 of 8 preoperative cases were histopathologically proven to be of benign etiology. 3 low grade and 2 high grade postoperative cases were disease free on 6 months follow-up. Tracer uptake was quantified by standardized uptake values (SUV(max)) and the SUV max ratio of tumor to normal symmetrical area of contra lateral hemisphere (T/N). 18F-FDOPA uptake was also quantified by SUV(max) ratio of tumor to striatum (T/S). Conventional MR studies were done in all patients.
Results: Both high-grade and low-grade tumors were well visualized with 18F-FDOPA PET. Sensitivity of 18F-FDOPA PET was substantially higher (6/6 preoperative, 3/3 low grade postoperative, 7/7 high grade postoperative) than with 18F-FDG (3/6 preoperative, 1/3 low grade postoperative, 3/7 high grade postoperative) and 13N-Ammonia PET (2/6 preoperative, 1/3 low grade postoperative, 1/7 high grade postoperative). FDOPA was equally specific as FDG and Ammonia PET in operated cases but was falsely positive in two preoperative cases. Sensitivity of FDOPA (16/16) was more than MRI (13/16).
Conclusion: 18F-FDG uptake correlates with tumor grade. Though 18F-FDOPA PET cannot distinguish between tumor grade, it is more reliable than 18F-FDG and 13N-Ammonia PET for evaluating brain tumors. 18F-FDOPA PET may prove to be superior to MRI in evaluating recurrence and residual tumor tissue. 13N-Ammonia PET did not show any encouraging results.
Keywords: 13N-Ammonia; 18F-FDG; 18F-FDOPA; MRI; PET; brain tumors; sensitivity.
Conflict of interest statement
Figures

Similar articles
-
Comparative study of (18)F-DOPA, (13)N-Ammonia and F18-FDG PET/CT in primary brain tumors.Indian J Nucl Med. 2011 Jul;26(3):139-43. doi: 10.4103/0972-3919.103996. Indian J Nucl Med. 2011. PMID: 23326065 Free PMC article.
-
18F-FDOPA PET imaging of brain tumors: comparison study with 18F-FDG PET and evaluation of diagnostic accuracy.J Nucl Med. 2006 Jun;47(6):904-11. J Nucl Med. 2006. PMID: 16741298 Clinical Trial.
-
Perfusion-metabolism coupling in recurrent gliomas: a prospective validation study with 13N-ammonia and 18F-fluorodeoxyglucose PET/CT.Neuroradiology. 2014 Oct;56(10):893-902. doi: 10.1007/s00234-014-1389-0. Epub 2014 Jul 3. Neuroradiology. 2014. PMID: 24989883
-
Current Radiopharmaceuticals for Positron Emission Tomography of Brain Tumors.Brain Tumor Res Treat. 2018 Oct;6(2):47-53. doi: 10.14791/btrt.2018.6.e13. Brain Tumor Res Treat. 2018. PMID: 30381916 Free PMC article. Review.
-
What Does PET Imaging Bring to Neuro-Oncology in 2022? A Review.Cancers (Basel). 2022 Feb 10;14(4):879. doi: 10.3390/cancers14040879. Cancers (Basel). 2022. PMID: 35205625 Free PMC article. Review.
Cited by
-
A Comparison of PET Tracers in Recurrent High-Grade Gliomas: A Systematic Review.Int J Mol Sci. 2022 Dec 27;24(1):408. doi: 10.3390/ijms24010408. Int J Mol Sci. 2022. PMID: 36613852 Free PMC article.
-
Diagnostic accuracy of magnetic resonance imaging techniques for treatment response evaluation in patients with high-grade glioma, a systematic review and meta-analysis.Eur Radiol. 2017 Oct;27(10):4129-4144. doi: 10.1007/s00330-017-4789-9. Epub 2017 Mar 22. Eur Radiol. 2017. PMID: 28332014 Free PMC article.
-
13N-NH3 PET/CT in oncological disease.Jpn J Radiol. 2019 Dec;37(12):799-807. doi: 10.1007/s11604-019-00883-7. Epub 2019 Oct 10. Jpn J Radiol. 2019. PMID: 31599383 Review.
-
Interrogating tumor metabolism and tumor microenvironments using molecular positron emission tomography imaging. Theranostic approaches to improve therapeutics.Pharmacol Rev. 2013 Sep 24;65(4):1214-56. doi: 10.1124/pr.113.007625. Print 2013. Pharmacol Rev. 2013. PMID: 24064460 Free PMC article. Review.
-
Diagnostic and grading accuracy of 18F-FDOPA PET and PET/CT in patients with gliomas: a systematic review and meta-analysis.BMC Cancer. 2019 Aug 5;19(1):767. doi: 10.1186/s12885-019-5938-0. BMC Cancer. 2019. PMID: 31382920 Free PMC article.
References
-
- Dooms GC, Hecht S, Brant-Zawadzki M, Berthiaume Y, Norman D, Newton TH. Brain radiation lesions: MR imaging. Radiology. 1986;15:149–55. - PubMed
-
- Van Dellen JR. Danziger A Failure of computerized tomography to differentiate between radiation necrosis and cerebral tumour. S Afr Med J. 1978;53:171–2. - PubMed
-
- Nelson SJ, Huhn S, Vigneron DB, Day MR, Wald LL, Prados M, et al. Volume MRI and MRSI techniques for the quantitation of treatment response in brain tumors: presentation of a detailed case study. J Magn Reson Imaging. 1997;7:1146–52. - PubMed
