

Arterial stiffness, central hemodynamics, and cardiovascular risk in hypertension
- PMID: 22174583
- PMCID: PMC3237102
- DOI: 10.2147/VHRM.S25270
Arterial stiffness, central hemodynamics, and cardiovascular risk in hypertension
Abstract
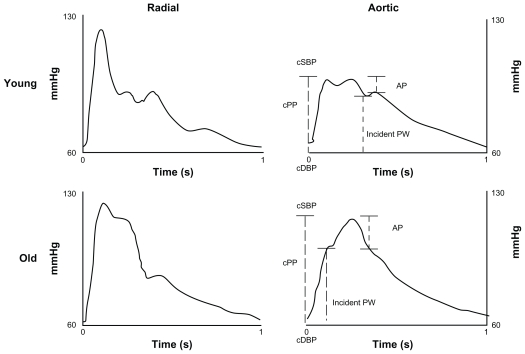
This review summarizes several scientific contributions at the recent Satellite Symposium of the European Society of Hypertension, held in Milan, Italy. Arterial stiffening and its hemodynamic consequences can be easily and reliably measured using a range of noninvasive techniques. However, like blood pressure (BP) measurements, arterial stiffness should be measured carefully under standardized patient conditions. Carotid-femoral pulse wave velocity has been proposed as the gold standard for arterial stiffness measurement and is a well recognized predictor of adverse cardiovascular outcome. Systolic BP and pulse pressure in the ascending aorta may be lower than pressures measured in the upper limb, especially in young individuals. A number of studies suggest closer correlation of end-organ damage with central BP than with peripheral BP, and central BP may provide additional prognostic information regarding cardiovascular risk. Moreover, BP-lowering drugs can have differential effects on central aortic pressures and hemodynamics compared with brachial BP. This may explain the greater beneficial effect provided by newer antihypertensive drugs beyond peripheral BP reduction. Although many methodological problems still hinder the wide clinical application of parameters of arterial stiffness, these will likely contribute to cardiovascular assessment and management in future clinical practice. Each of the abovementioned parameters reflects a different characteristic of the atherosclerotic process, involving functional and/or morphological changes in the vessel wall. Therefore, acquiring simultaneous measurements of different parameters of vascular function and structure could theoretically enhance the power to improve risk stratification. Continuous technological effort is necessary to refine our methods of investigation in order to detect early arterial abnormalities. Arterial stiffness and its consequences represent the great challenge of the twenty-first century for affluent countries, and "de-stiffening" will be the goal of the next decades.
Keywords: arterial elasticity; central blood pressure; compliance; pulse wave velocity; stiffness.
Figures
Similar articles
-
Aortic stiffness and central hemodynamics in treatment-naïve HIV infection: a cross-sectional study.BMC Cardiovasc Disord. 2020 Oct 7;20(1):440. doi: 10.1186/s12872-020-01722-8. BMC Cardiovasc Disord. 2020. PMID: 33028211 Free PMC article.
-
Clinical measurement of arterial stiffness obtained from noninvasive pressure waveforms.Am J Hypertens. 2005 Jan;18(1 Pt 2):3S-10S. doi: 10.1016/j.amjhyper.2004.10.009. Am J Hypertens. 2005. PMID: 15683725 Review.
-
Aortic Hemodynamics and Arterial Stiffness Responses to Muscle Metaboreflex Activation With Concurrent Cold Pressor Test.Am J Hypertens. 2015 Nov;28(11):1332-8. doi: 10.1093/ajh/hpv043. Epub 2015 Apr 22. Am J Hypertens. 2015. PMID: 25904650 Clinical Trial.
-
Clinical relevance of aortic stiffness in end-stage renal disease and diabetes: implication for hypertension management.J Hypertens. 2018 Jun;36(6):1237-1246. doi: 10.1097/HJH.0000000000001665. J Hypertens. 2018. PMID: 29300243 Review.
-
Role of antihypertensive drugs in arterial 'de-stiffening' and central pulsatile hemodynamics.Am J Cardiovasc Drugs. 2012 Jun 1;12(3):143-56. doi: 10.2165/11599040-000000000-00000. Am J Cardiovasc Drugs. 2012. PMID: 22540323 Review.
Cited by
-
Central Hypertension in Patients With Thoracic Aortic Aneurysms: Prevalence and Association With Aneurysm Size and Growth.Am J Hypertens. 2022 Jan 5;35(1):79-86. doi: 10.1093/ajh/hpaa183. Am J Hypertens. 2022. PMID: 33759993 Free PMC article.
-
Rationale and study design of the Prospective comparison of Angiotensin Receptor neprilysin inhibitor with Angiotensin receptor blocker MEasuring arterial sTiffness in the eldERly (PARAMETER) study.BMJ Open. 2014 Feb 4;4(2):e004254. doi: 10.1136/bmjopen-2013-004254. BMJ Open. 2014. PMID: 24496699 Free PMC article. Clinical Trial.
-
Chronic p38 mitogen-activated protein kinase inhibition improves vascular function and remodeling in angiotensin II-dependent hypertension.J Renin Angiotensin Aldosterone Syst. 2016 Jul 12;17(3):1470320316653284. doi: 10.1177/1470320316653284. Print 2016 Jul. J Renin Angiotensin Aldosterone Syst. 2016. PMID: 27407119 Free PMC article.
-
Perceived Control Predicts Pulse Pressure in African American Men: The Baltimore Study of Black Aging.Ethn Dis. 2015 Aug 7;25(3):263-70. doi: 10.18865/ed.25.3.263. Ethn Dis. 2015. PMID: 26676156 Free PMC article.
-
Pulmonary Function and Arterial Stiffness in Chronic Heart Failure.Biomed Res Int. 2016;2016:5478394. doi: 10.1155/2016/5478394. Epub 2016 Dec 21. Biomed Res Int. 2016. PMID: 28097138 Free PMC article.
References
-
- Grzybowski A, Sak J, Pawlikowski J. 500th anniversary of the birth of the precursor of modern cardiology: Josephus Struthius Polonus 1510–1568. Cardiol J. 2011;18(5):581–586. - PubMed
-
- Blacher J, Guerin AP, Pannier B, et al. Impact of aortic stiffness on survival in end-stage renal disease. Circulation. 1999;99(18):2434–2439. - PubMed
-
- Laurent S, Boutouyrie P, Asmar R, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37(5):1236–1241. - PubMed
-
- Meaume S, Benetos A, Henry OF, et al. Aortic pulse wave velocity predicts cardiovascular mortality in subjects >70 years of age. Arterioscler Thromb Vasc Biol. 2001;21(12):2046–2050. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
