

Fatty Acid binding protein 4 is associated with carotid atherosclerosis and outcome in patients with acute ischemic stroke
- PMID: 22174896
- PMCID: PMC3235157
- DOI: 10.1371/journal.pone.0028785
Fatty Acid binding protein 4 is associated with carotid atherosclerosis and outcome in patients with acute ischemic stroke
Abstract
Background and purpose: Fatty acid binding protein 4 (FABP4) has been shown to play an important role in macrophage cholesterol trafficking and associated inflammation. To further elucidate the role of FABP4 in atherogenesis in humans, we examined the regulation of FABP4 in carotid atherosclerosis and ischemic stroke.
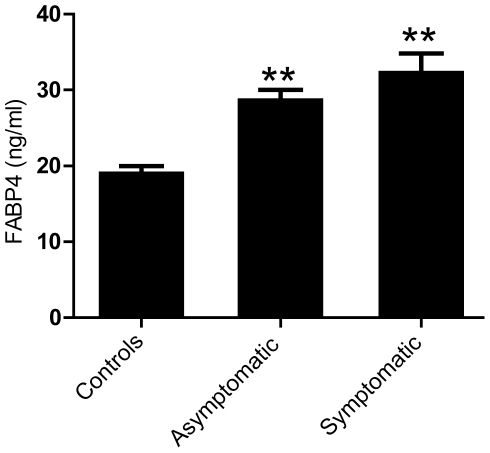
Methods: We examined plasma FABP4 levels in asymptomatic (n = 28) and symptomatic (n = 31) patients with carotid atherosclerosis, as well as in 202 subjects with acute ischemic stroke. In a subgroup of patients we also analysed the expression of FABP4 within the atherosclerotic lesion. In addition, we investigated the ability of different stimuli with relevance to atherosclerosis to regulate FABP4 expression in monocytes/macrophages.
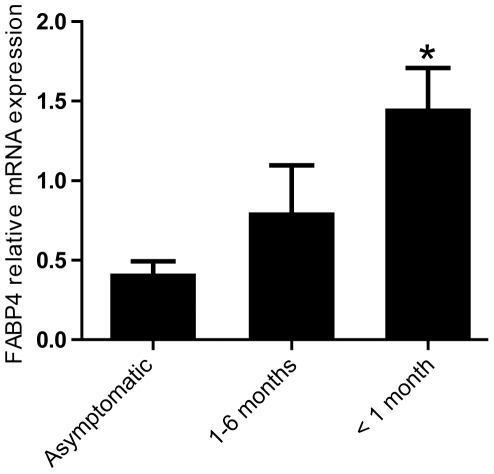
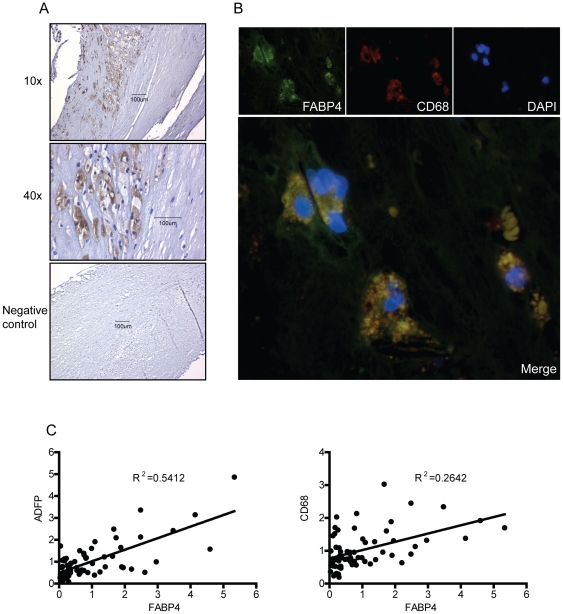
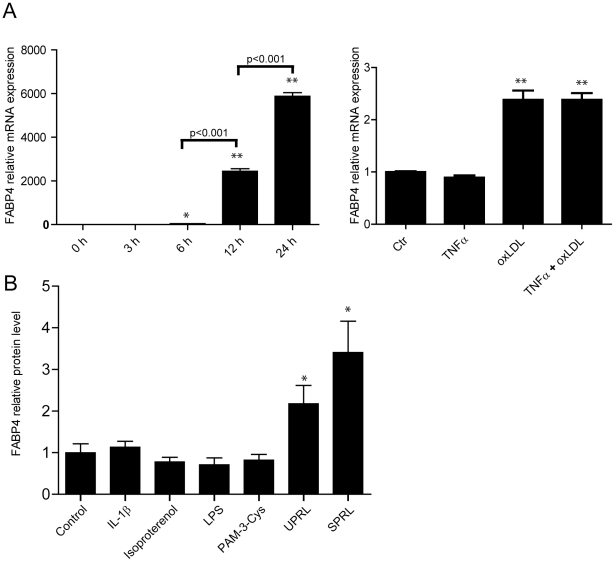
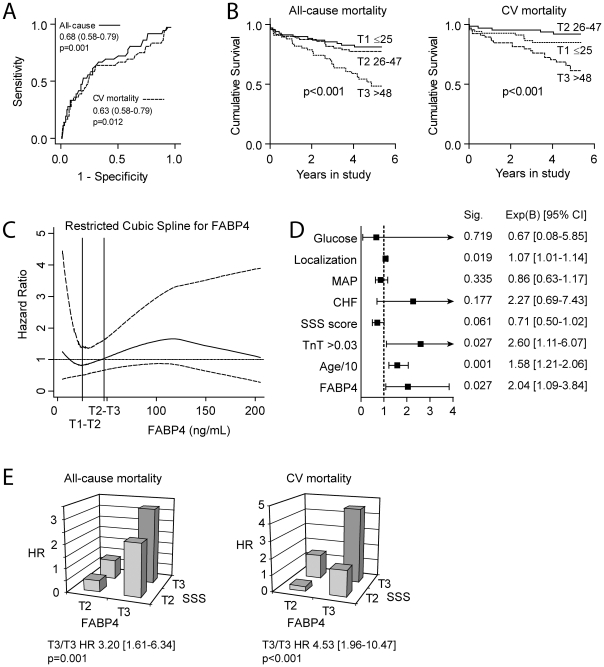
Results: FABP4 levels were higher in patients with carotid atherosclerosis, both systemically and within the atherosclerotic lesion, with particular high mRNA levels in carotid plaques from patients with the most recent symptoms. Immunostaining of carotid plaques localized FABP4 to macrophages, while activated platelets and oxidized LDL were potent stimuli for FABP4 expression in monocytes/macrophages in vitro. When measured at the time of acute ischemic stroke, high plasma levels of FABP4 were significantly associated with total and cardiovascular mortality during follow-up, although we did not find that addition of FABP4 to the fully adjusted multivariate model had an effect on the prognostic discrimination for all-cause mortality as assessed by c-statistics.
Conclusions: FABP4 is linked to atherogenesis, plaque instability and adverse outcome in patients with carotid atherosclerosis and acute ischemic stroke.
Conflict of interest statement
Figures
References
-
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352:1685–1695. - PubMed
-
- Halvorsen B, Otterdal K, Dahl TB, Skjelland M, Gullestad L, et al. Atherosclerotic plaque stability--what determines the fate of a plaque? Prog Cardiovasc Dis. 2008;51:183–194. - PubMed
-
- Hotamisligil GS, Johnson RS, Distel RJ, Ellis R, Papaioannou VE, et al. Uncoupling of obesity from insulin resistance through a targeted mutation in aP2, the adipocyte fatty acid binding protein. Science. 1996;274:1377–1379. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
