

Predicting functional status following amputation after lower extremity bypass
- PMID: 22176876
- PMCID: PMC3339378
- DOI: 10.1016/j.avsg.2011.07.014
Predicting functional status following amputation after lower extremity bypass
Abstract
Background: Some patients who undergo lower extremity bypass (LEB) for critical limb ischemia ultimately require amputation. The functional outcome achieved by these patients after amputation is not well known. Therefore, we sought to characterize the functional outcome of patients who undergo amputation after LEB, and to describe the pre- and perioperative factors associated with independent ambulation at home after lower extremity amputation.
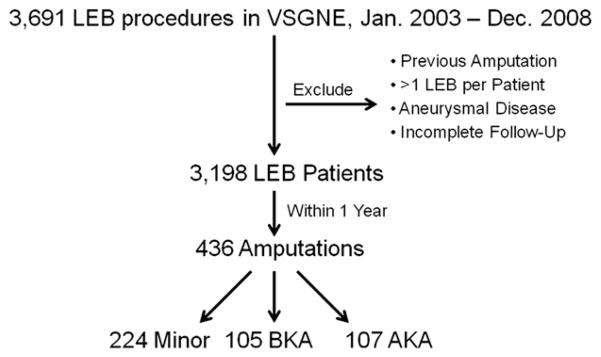
Methods: Within a cohort of 3,198 patients who underwent an LEB between January, 2003 and December, 2008, we studied 436 patients who subsequently received an above-knee (AK), below-knee (BK), or minor (forefoot or toe) ipsilateral or contralateral amputation. Our main outcome measure consisted of a "good functional outcome," defined as living at home and ambulating independently. We calculated univariate and multivariate associations among patient characteristics and our main outcome measure, as well as overall survival.
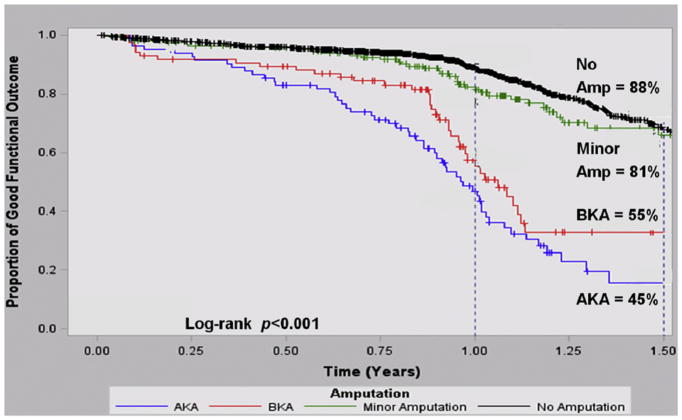
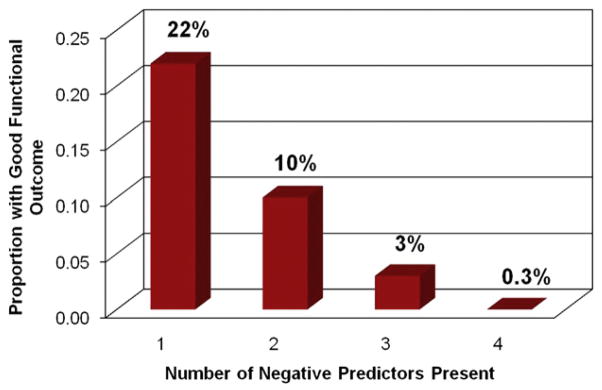
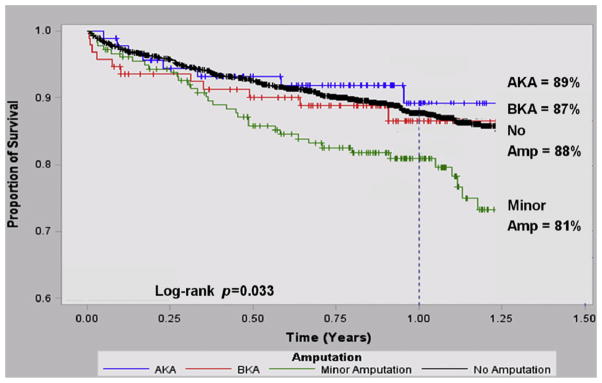
Results: Of the 436 patients who underwent amputation within the first year following LEB, 224 of 436 (51.4%) had a minor amputation, 105 of 436 (24.1%) had a BK amputation, and 107 of 436 (24.5%) had an AK amputation. The majority of AK (75 of 107, 72.8%) and BK amputations (72 of 105, 70.6%) occurred in the setting of bypass graft thrombosis, whereas nearly all minor amputations (200 of 224, 89.7%) occurred with a patent bypass graft. By life-table analysis at 1 year, we found that the proportion of surviving patients with a good functional outcome varied by the presence and extent of amputation (proportion surviving with good functional outcome = 88% no amputation, 81% minor amputation, 55% BK amputation, and 45% AK amputation, p = 0.001). Among those analyzed at long-term follow-up, survival was slightly lower for those who had a minor amputation when compared with those who did not receive an amputation after LEB (81 vs. 88%, p = 0.02). Survival among major amputation patients did not significantly differ compared with no amputation (BK amputation 87%, p = 0.14, AK amputation 89%, p = 0.27); however, this part of the analysis was limited by its sample size (n = 212). In multivariable analysis, we found that the patients most likely to remain ambulatory and live independently despite undergoing a lower extremity amputation were those living at home preoperatively (hazard ratio [HR]: 6.8, 95% confidence interval [CI]: 0.94-49, p = 0.058) and those with preoperative statin use (HR: 1.6, 95% CI: 1.2-2.1, p = 0.003), whereas the presence of several comorbidities identified patients less likely to achieve a good functional outcome: coronary disease (HR: 0.6, 95% CI: 0.5-0.9, p = 0.003), dialysis (HR: 0.5, 95% CI: 0.3-0.9, p = 0.02), and congestive heart failure (HR: 0.5, 95% CI: 0.3-0.8, p = 0.005).
Conclusions: A postoperative amputation at any level impacts functional outcomes following LEB surgery, and the extent of amputation is directly related to the effect on functional outcome. It is possible, based on preoperative patient characteristics, to identify patients undergoing LEB who are most or least likely to achieve good functional outcomes even if a major amputation is ultimately required. These findings may assist in patient education and surgical decision making in patients who are poor candidates for lower extremity bypass.
Published by Elsevier Inc.
Figures
References
-
- Egorova NN, Guillerme S, Gelijns A, et al. An analysis of the outcomes of a decade of experience with lower extremity revascularization including limb salvage, lengths of stay, and safety. J Vasc Surg. 2010;51:878–885.e1. - PubMed
-
- Goodney PP, Beck AW, Nagle J, Welch HG, Zwolak RM. National trends in lower extremity bypass surgery, endovascular interventions, and major amputations. J Vasc Surg. 2009;50:54–60. - PubMed
-
- Landry GJ. Functional outcome of critical limb ischemia. J Vasc Surg. 2007;45:A141–A148. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
