

Validation of proposed DSM-5 criteria for autism spectrum disorder
- PMID: 22176937
- PMCID: PMC3244681
- DOI: 10.1016/j.jaac.2011.09.021
Validation of proposed DSM-5 criteria for autism spectrum disorder
Abstract
Objective: The primary aim of the present study was to evaluate the validity of proposed DSM-5 criteria for autism spectrum disorder (ASD).
Method: We analyzed symptoms from 14,744 siblings (8,911 ASD and 5,863 non-ASD) included in a national registry, the Interactive Autism Network. Youth 2 through 18 years of age were included if at least one child in the family was diagnosed with ASD. Caregivers reported symptoms using the Social Responsiveness Scale and the Social Communication Questionnaire. The structure of autism symptoms was examined using latent variable models that included categories, dimensions, or hybrid models specifying categories and subdimensions. Diagnostic efficiency statistics evaluated the proposed DSM-5 algorithm in identifying ASD.
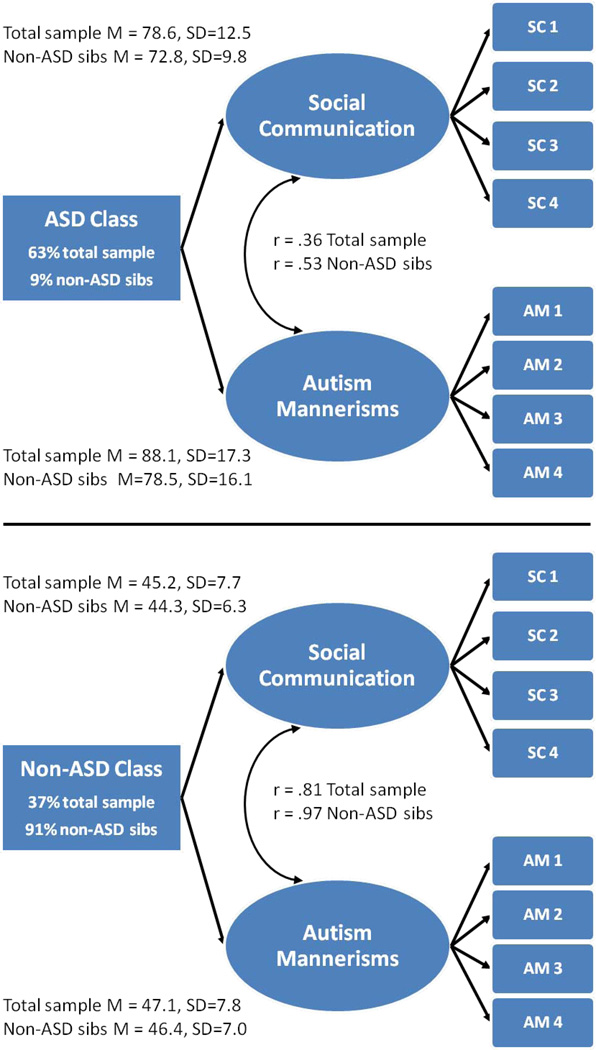
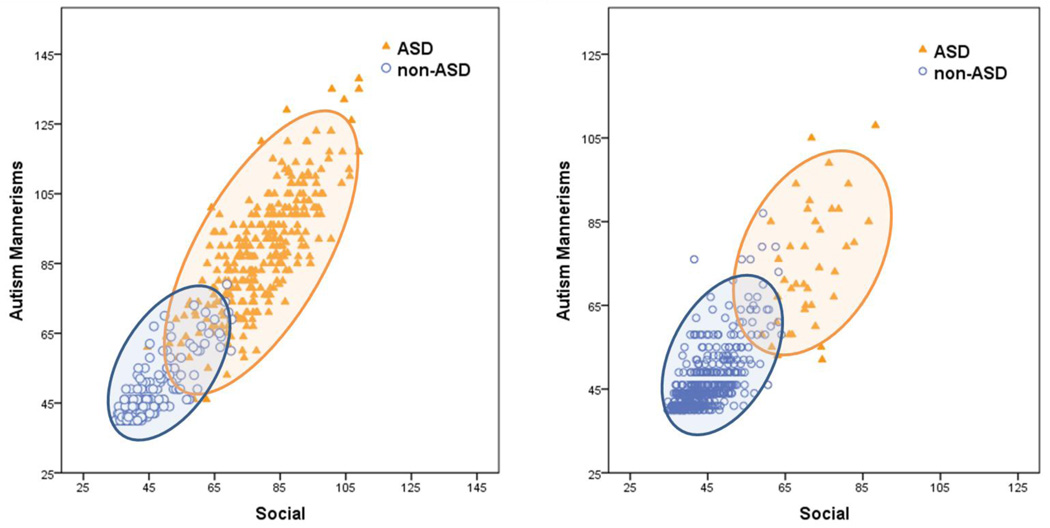
Results: A hybrid model that included both a category (ASD versus non-ASD) and two symptom dimensions (social communication/interaction and restricted/repetitive behaviors) was more parsimonious than all other models and replicated across measures and subsamples. Empirical classifications from this hybrid model closely mirrored clinical ASD diagnoses (90% overlap), implying a broad ASD category distinct from non-ASD. DSM-5 criteria had superior specificity relative to DSM-IV-TR criteria (0.97 versus 0.86); however sensitivity was lower (0.81 versus 0.95). Relaxing DSM-5 criteria by requiring one less symptom criterion increased sensitivity (0.93 versus 0.81), with minimal reduction in specificity (0.95 versus 0.97).
Conclusions: Results supported the validity of proposed DSM-5 criteria for ASD as provided in Phase I Field Trials criteria. Increased specificity of DSM-5 relative to DSM-IV-TR may reduce false positive diagnoses, a particularly relevant consideration for low base rate clinical settings. Phase II testing of DSM-5 should consider a relaxed algorithm, without which as many as 12% of ASD-affected individuals, particularly females, will be missed. Relaxed DSM-5 criteria may improve identification of ASD, decreasing societal costs through appropriate early diagnosis and maximizing intervention resources.
Copyright © 2012 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure: Drs. Law, Speer, Eng, and Hardan, and Mrs. Embacher report no biomedical financial interests or potential conflicts of interest.
Figures

Comment in
-
Lumpers and splitters: who knows? Who cares?J Am Acad Child Adolesc Psychiatry. 2012 Jan;51(1):6-7. doi: 10.1016/j.jaac.2011.10.009. J Am Acad Child Adolesc Psychiatry. 2012. PMID: 22176934 No abstract available.
References
-
- Fombonne E. Epidemiology of pervasive developmental disorders. Pediatr. Res. Jun. 2009;65(6):591–598. - PubMed
-
- Ganz ML. The lifetime distribution of incremental societal costs of autism. Arch. Pediatr. Adolesc. Med. 2007;161:343–349. - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Fourth Edition. Washington, DC: American Psychiatric Association; 2000. Text Revision.
-
- DSM-5 Development. 299.00 Autistic Disorder. [Accessed February 01, 2011];2011 http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=94.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
