

A pragmatic multi-centre randomised controlled trial of fluid loading in high-risk surgical patients undergoing major elective surgery--the FOCCUS study
- PMID: 22177541
- PMCID: PMC3388651
- DOI: 10.1186/cc10592
A pragmatic multi-centre randomised controlled trial of fluid loading in high-risk surgical patients undergoing major elective surgery--the FOCCUS study
Abstract
Introduction: Fluid strategies may impact on patient outcomes in major elective surgery. We aimed to study the effectiveness and cost-effectiveness of pre-operative fluid loading in high-risk surgical patients undergoing major elective surgery.
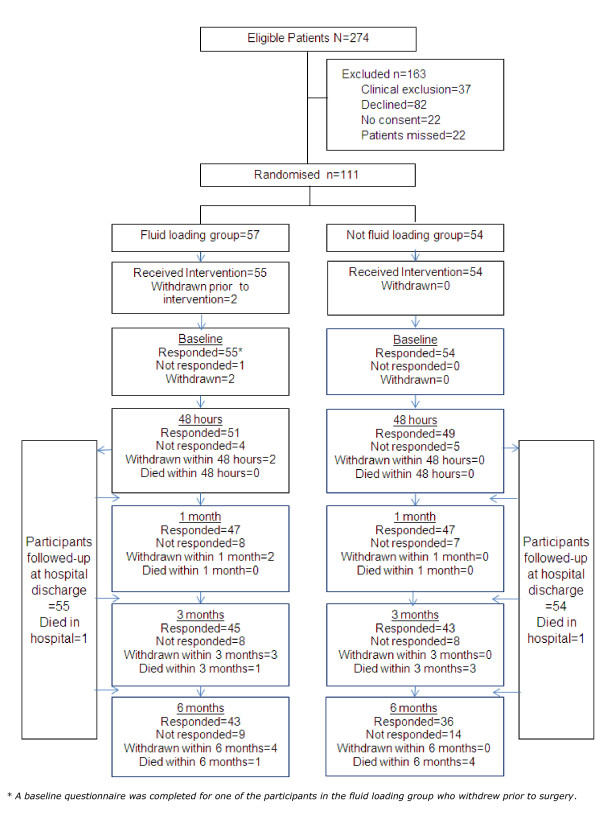
Methods: This was a pragmatic, non-blinded, multi-centre, randomised, controlled trial. We sought to recruit 128 consecutive high-risk surgical patients undergoing major abdominal surgery. The patients underwent pre-operative fluid loading with 25 ml/kg of Ringer's solution in the six hours before surgery. The control group had no pre-operative fluid loading. The primary outcome was the number of hospital days after surgery with cost-effectiveness as a secondary outcome.
Results: A total of 111 patients were recruited within the study time frame in agreement with the funder. The median pre-operative fluid loading volume was 1,875 ml (IQR 1,375 to 2,025) in the fluid group compared to 0 (IQR 0 to 0) in controls with days in hospital after surgery 12.2 (SD 11.5) days compared to 17.4 (SD 20.0) and an adjusted mean difference of 5.5 days (median 2.2 days; 95% CI -0.44 to 11.44; P = 0.07). There was a reduction in adverse events in the fluid intervention group (P = 0.048) and no increase in fluid based complications. The intervention was less costly and more effective (adjusted average cost saving: £2,047; adjusted average gain in benefit: 0.0431 quality adjusted life year (QALY)) and has a high probability of being cost-effective.
Conclusions: Pre-operative intravenous fluid loading leads to a non-significant reduction in hospital length of stay after high-risk major surgery and is likely to be cost-effective. Confirmatory work is required to determine whether these effects are reproducible, and to confirm whether this simple intervention could allow more cost-effective delivery of care.
Trial registration: Prospective Clinical Trials, ISRCTN32188676.
Figures
Comment in
-
Pragmatic fluid optimization in high-risk surgery patients: when pragmatism dilutes the benefits.Crit Care. 2012 Jan 31;16(1):106. doi: 10.1186/cc10604. Crit Care. 2012. PMID: 22410167 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
