

CCL5-independent helper T lymphocyte responses to immuno-dominant pneumococcal surface protein A epitopes
- PMID: 22178100
- PMCID: PMC3269505
- DOI: 10.1016/j.vaccine.2011.12.020
CCL5-independent helper T lymphocyte responses to immuno-dominant pneumococcal surface protein A epitopes
Abstract
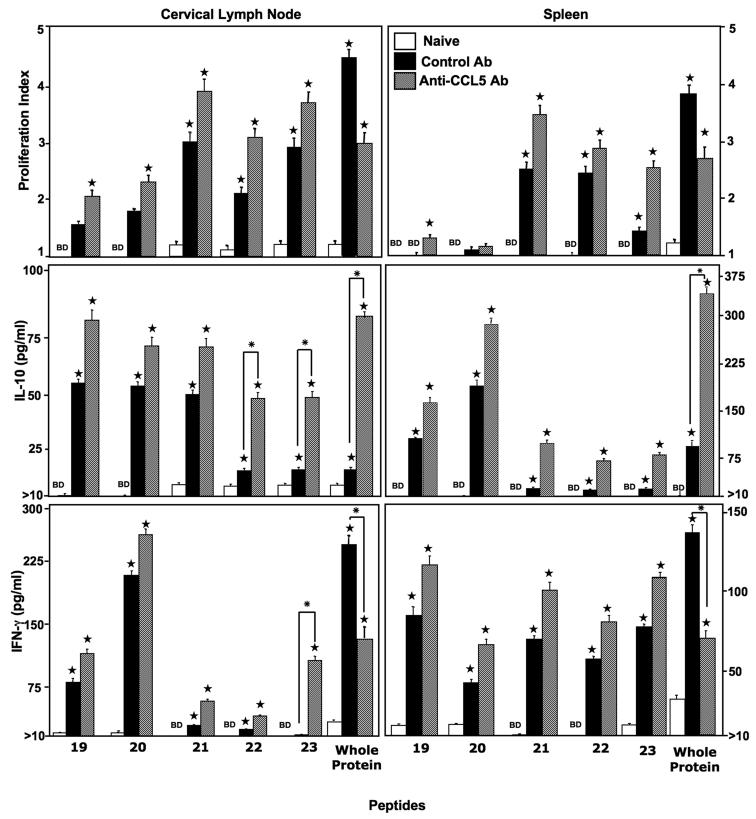
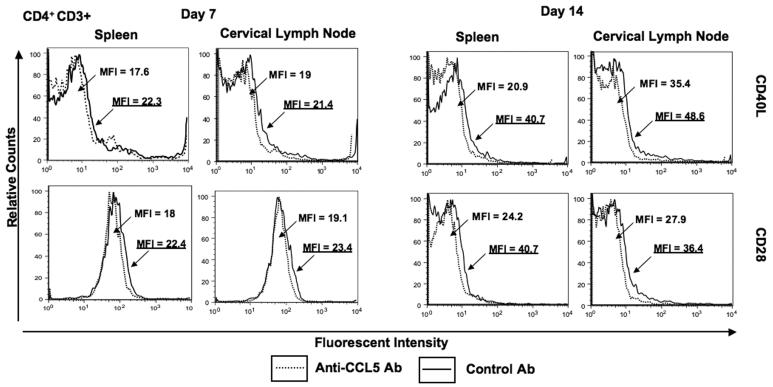
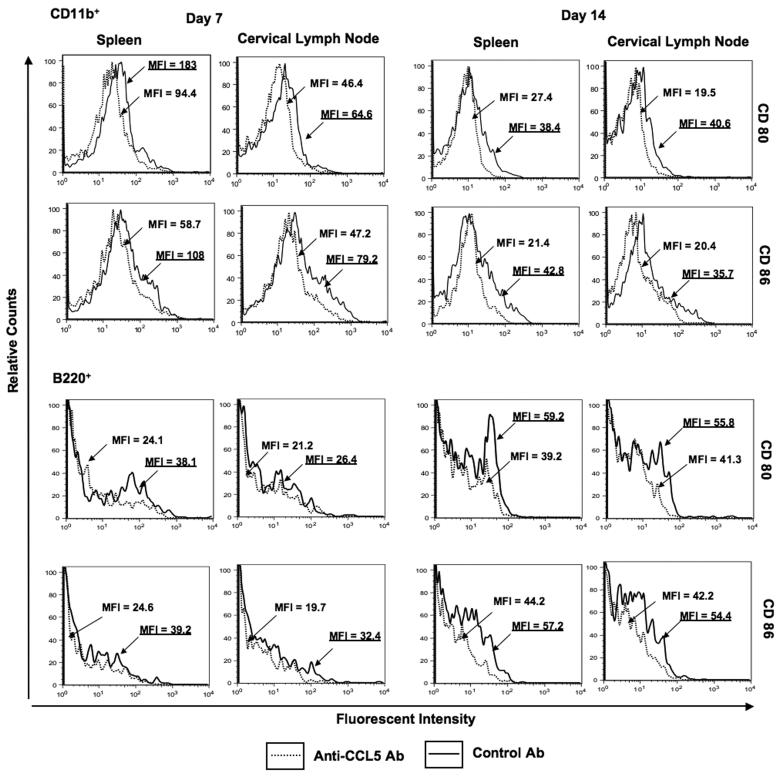
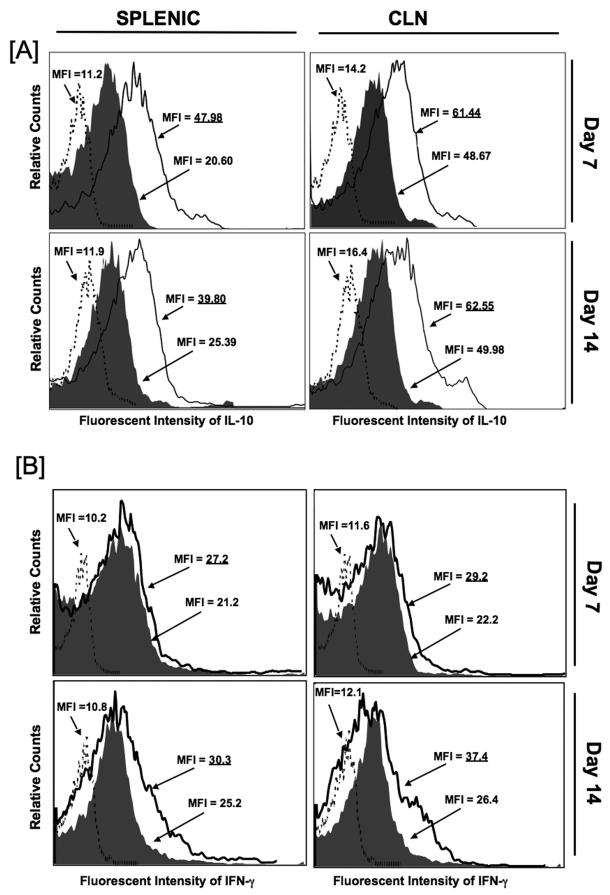
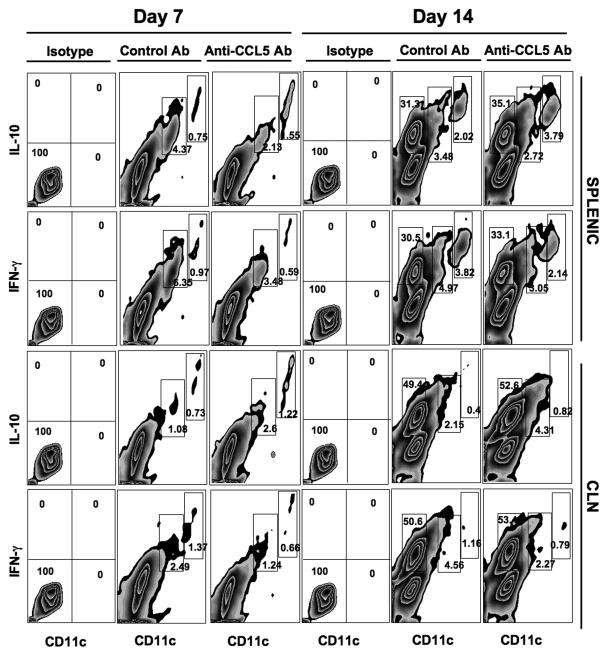
Understanding the requirements for protection against pneumococcal carriage and pneumonia will greatly benefit efforts in controlling these diseases. Several antigens, in addition to the polysaccharide capsule, have been implicated in both the virulence and protective immunity against Streptococcus pneumoniae; one of the best-studied S. pneumoniae antigens is pneumococcal surface protein A (PspA). Recently, it was shown that genetic polymorphisms could diminish CCL5 expression, which results in increased susceptibility to and progression of infectious diseases. We previously showed CCL5 blockade reduced PspA-specific humoral and cellular pneumococcal immunity, during S. pneumoniae strain EF3030-induced carriage, by diminishing IFN-γ and enhancing IL-10 secretion by effector T cells. We also identified immuno-dominant helper T lymphocyte (HTL) epitopes in PspA peptide 19-23 (PspA(199-246)), which caused comparatively more cytokine secretion and proliferation responses by splenic and cervical lymph node (CLN) CD4(+) T cells from mice previously challenged with S. pneumoniae strain EF3030. In this study, we sought to determine if PspA(199-246)-specific CD4(+) T cells responses were resistant to the effect of CCL5 deficiency. In short, T cell responses against these HTL epitopes were resistant to CCL5 inhibition, than compared to cells from control or naïve mice, and unaffected by reduced co-stimulatory molecule expression caused by CCL5 blockade. CCL5 deficiency also corresponded with a higher number of IL-10(+) CD11b(+) CD11c(Lo) and CD11b(+) CD11c(Hi) cells and lower IFN-γ expression by similar cells, than compared to controls. These data confirm CCL5 is an essential factor for optimal pneumococcal adaptive immunity and show CD4(+) T cell responses to PspA(199-246) are largely resistant to CCL5 deficiency.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Dagan R. Impact of pneumococcal conjugate vaccine on infections caused by antibiotic-resistant Streptococcus pneumoniae. Clin Microbiol Infect. 2009;3:16–20. - PubMed
-
- Dagan R, Givon-Lavi N, Leibovitz E, Greenberg D, Porat N. Introduction and proliferation of multidrug-resistant Streptococcus pneumoniae serotype 19A clones that cause acute otitis media in an unvaccinated population. J Infect Dis. 2009;199:776–85. - PubMed
-
- Reinert RR. The public health ramifications of pneumococcal resistance. Clin Microbiol Infect. 2009;3:1–3. - PubMed
-
- Lillard JW, Jr., Boyaka PN, Hedrick JA, Zlotnik A, McGhee JR. Lymphotactin acts as an innate mucosal adjuvant. J Immunol. 1999;162:1959–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
