

Field cancerization in the intestinal epithelium of patients with Crohn's ileocolitis
- PMID: 22178590
- PMCID: PMC4446968
- DOI: 10.1053/j.gastro.2011.12.004
Field cancerization in the intestinal epithelium of patients with Crohn's ileocolitis
Abstract
Background & aims: Tumors that develop in patients with Crohn's disease tend be multifocal, so field cancerization (the replacement of normal cells with nondysplastic but tumorigenic clones) might contribute to intestinal carcinogenesis. We investigated patterns of tumor development from pretumor intestinal cell clones.
Methods: We performed genetic analyses of multiple areas of intestine from 10 patients with Crohn's disease and intestinal neoplasia. Two patients had multifocal neoplasia; longitudinal sections were collected from 3 patients. Individual crypts were microdissected and genotyped; clonal dependency analysis was used to determine the order and timing of mutations that led to tumor development.
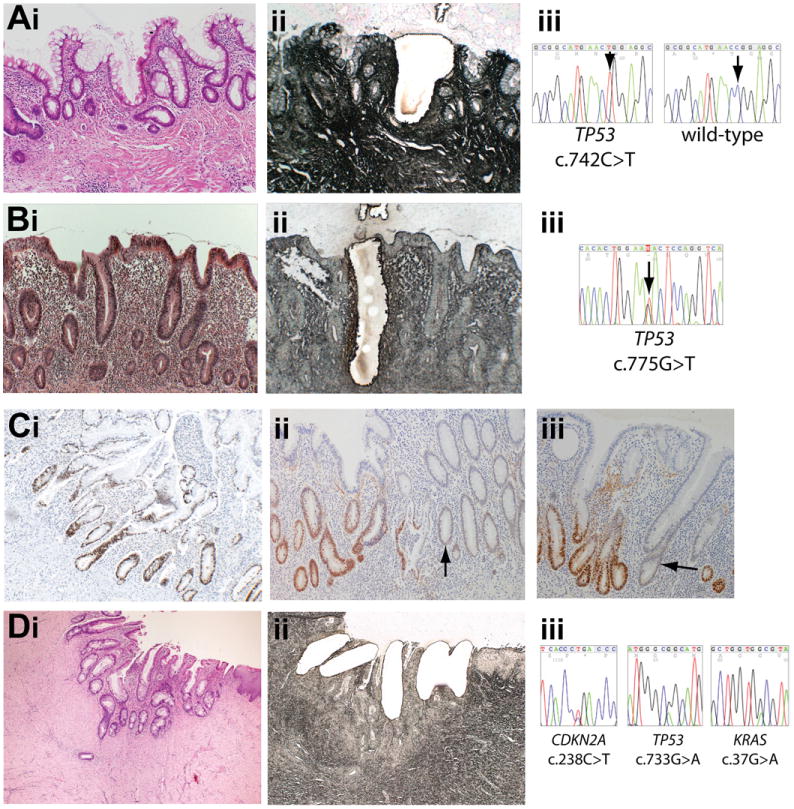
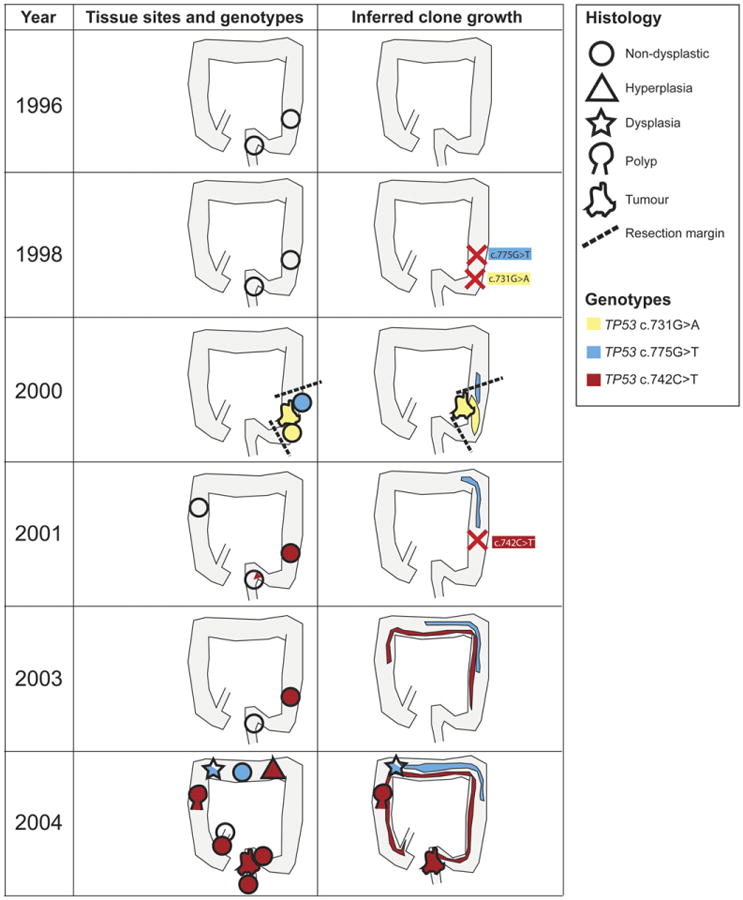
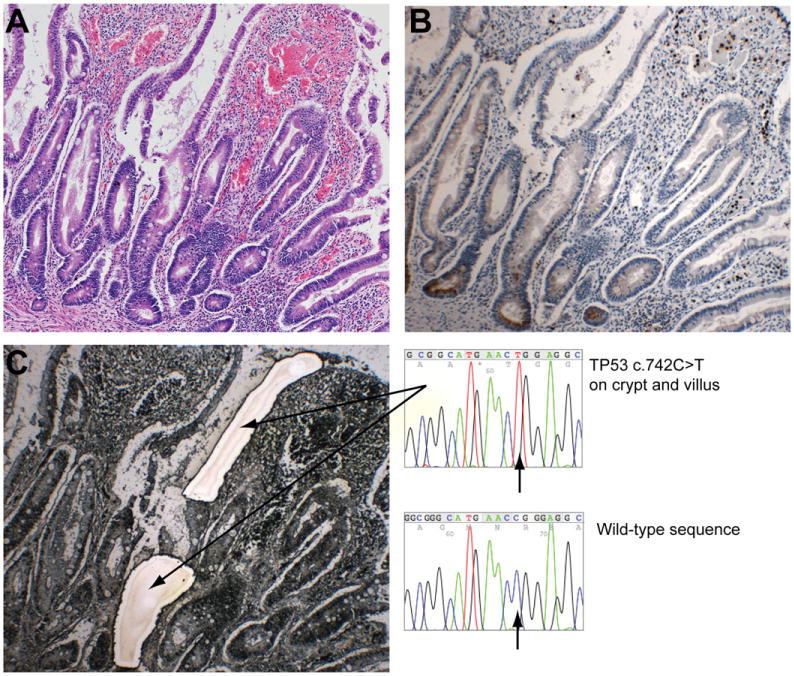
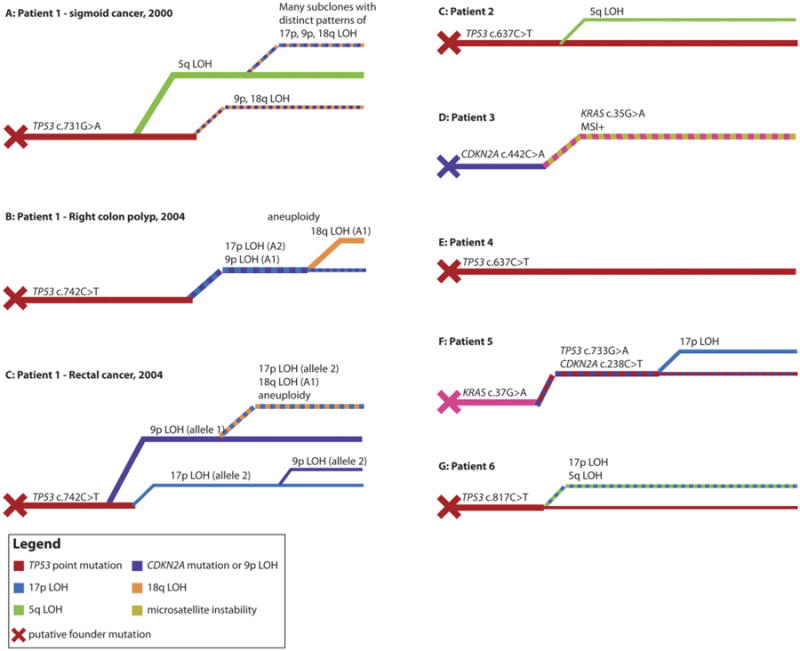
Results: The same mutations in KRAS, CDKN2A(p16), and TP53 that were observed in neoplasias were also present in nontumor, nondysplastic, and dysplastic epithelium. In 2 patients, carcinogenic mutations were detected in nontumor epithelium 4 years before tumors developed. The same mutation (TP53 p.R248W) was detected at multiple sites along the entire length of the colon from 1 patient; it was the apparent founder mutation for synchronous tumors and multiple dysplastic areas. Disruption of TP53, CDKN2A, and KRAS were all seen as possible initial events in tumorigenesis; the sequence of mutations (the tumor development pathway) differed among lesions.
Conclusions: Pretumor clones can grow extensively in the intestinal epithelium of patients with Crohn's disease. Segmental resections for neoplasia in patients with Crohn's disease might therefore leave residual pretumor disease, and dysplasia might be an unreliable biomarker for cancer risk. Characterization of the behavior of pretumor clones might be used to predict the development of intestinal neoplasia.
Copyright © 2012 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Laukoetter MG, Mennigen R, Hannig CM, et al. Intestinal cancer risk in Crohn's disease: a meta-analysis. J Gastrointest Surg. 2011;15:576–583. - PubMed
-
- Hemminki K, Li X, Sundquist J, et al. Cancer risks in Crohn disease patients. Ann Oncol. 2009;20:574–580. - PubMed
-
- von Roon AC, Reese G, Teare J, et al. The risk of cancer in patients with Crohn's disease. Dis Colon Rectum. 2007;50:839–855. - PubMed
-
- Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohn's disease. Aliment Pharmacol Ther. 2006;23:1097–1104. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
