

Multiple myeloma: 2012 update on diagnosis, risk-stratification, and management
- PMID: 22180161
- PMCID: PMC3629949
- DOI: 10.1002/ajh.22237
Multiple myeloma: 2012 update on diagnosis, risk-stratification, and management
Erratum in
- Am J Hematol. 2012 Apr;87(4):452
- Am J Hematol. 2014 Jun;89(6):669
Abstract
Disease overview: Multiple myeloma accounts for ∼10% of all hematologic malignancies.
Diagnosis: The diagnosis requires 10% or more clonal plasma cells on bone marrow examination or a biopsy proven plasmacytoma plus evidence of end-organ damage felt to be related to the underlying plasma-cell disorder.
Risk stratification: Patients with 17p deletion, t(14;16), t(14;20), or high-risk gene expression profiling signature have high-risk myeloma. Patients with t(4;14) translocation, karyotypic deletion 13, or hypodiploidy are considered to have intermediate-risk disease. All others are considered to have standard-risk myeloma.
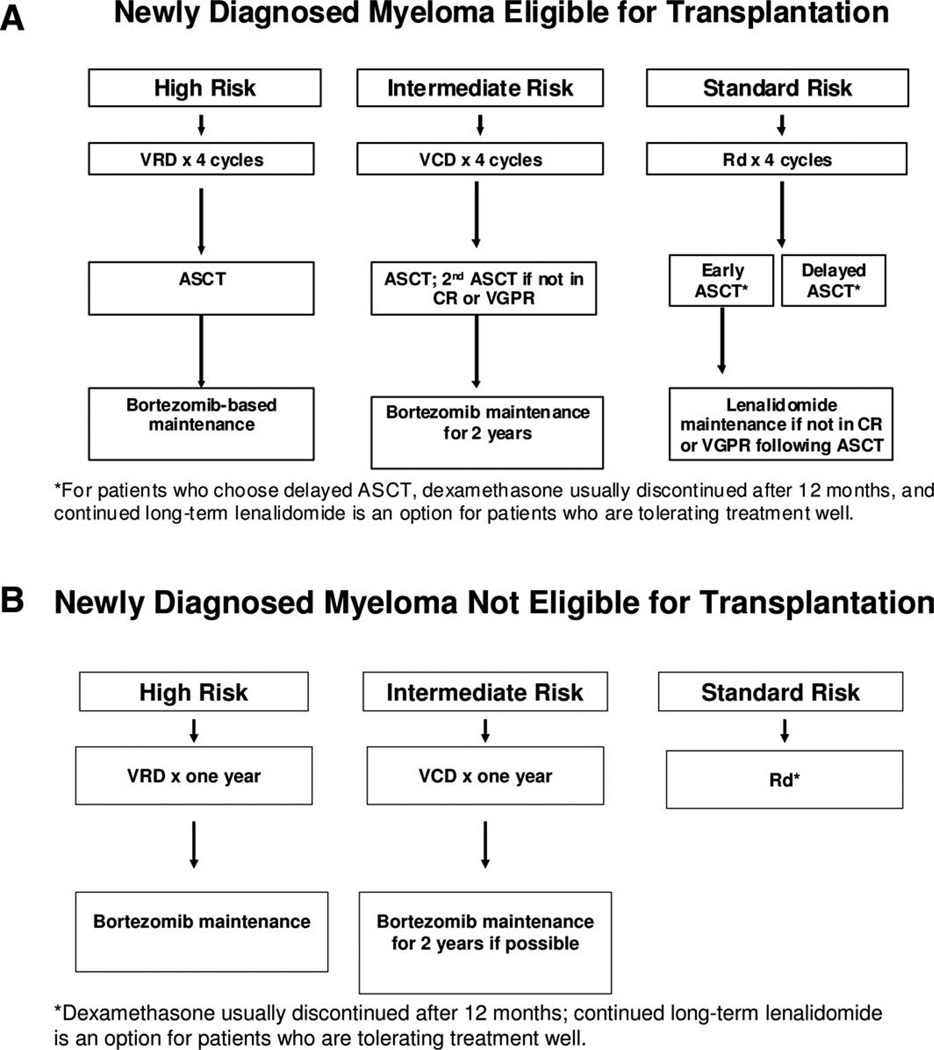
Risk-adapted therapy: Standard-risk patients are treated with nonalkylator-based therapy such as lenalidomide plus low-dose dexamethasone (Rd) followed by autologous stem-cell transplantation (ASCT). An alternative strategy is to continue initial therapy after stem-cell collection, reserving ASCT for first relapse. Intermediate-risk and high-risk patients are treated with a bortezomib-based induction followed by ASCT and then bortezomib-based maintenance. Patients not eligible for ASCT can be treated with Rd for standard risk disease, or with a bortezomib-based regimen if intermediate-risk or high-risk features are present. To reduce toxicity, when using bortezomib, the once-weekly subcutaneous dose is preferred; similarly, when using dexamethasone, the low-dose approach (40 mg once a week) is preferred, unless there is a need for rapid disease control.
Management of refractory disease: Patients with indolent relapse can be treated first with two-drug or three-drug combinations. Patients with more aggressive relapse often require therapy with a combination of multiple active agents. The most promising new agents in development are pomalidomide and carfilizomib.
Copyright © 2011 Wiley Periodicals, Inc.
Conflict of interest statement
Conflict of interest: Nothing to report
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Kyle RA, Therneau TM, Rajkumar SV, Larson DR, Plevak MF, Melton LJ., III Incidence of multiple myeloma in Olmsted County, Minnesota: Trend over 6 decades. Cancer. 2004;101:2667–2674. - PubMed
-
- Landgren O, Weiss BM. Patterns of monoclonal gammopathy of undetermined significance and multiple myeloma in various ethnic/racial groups: Support for genetic factors in pathogenesis. Leukemia. 2009;23:1691–1697. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous