

Porcine subintestinal submucosal graft augmentation for rectocele repair: a randomized controlled trial
- PMID: 22183220
- PMCID: PMC3244827
- DOI: 10.1097/AOG.0b013e31823d407e
Porcine subintestinal submucosal graft augmentation for rectocele repair: a randomized controlled trial
Abstract
Objective: To estimate the effect of porcine subintestinal submucosal graft augmentation on improving anatomic and subjective rectocele repair outcomes compared with native tissue repair.
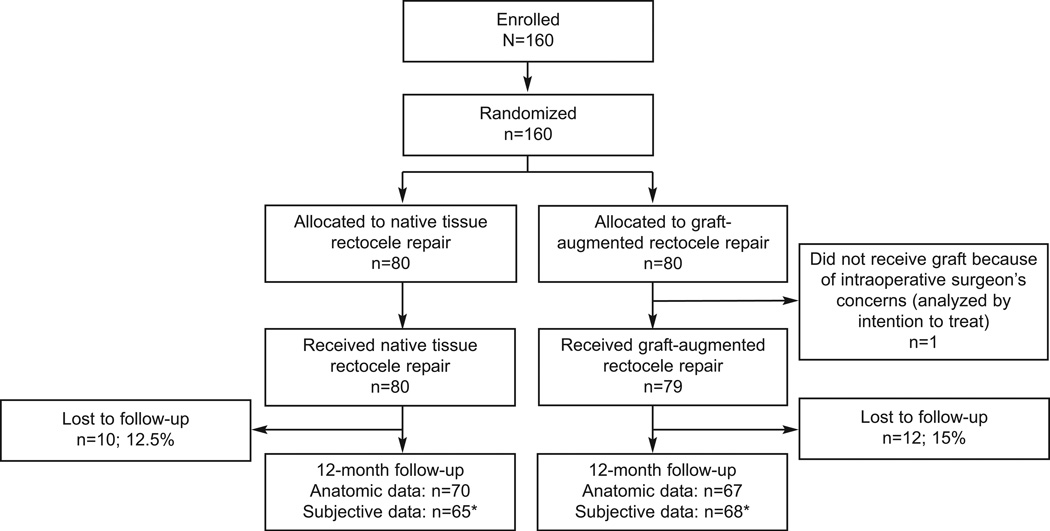
Methods: We conducted a randomized controlled trial at two sites, including women with at least stage 2 symptomatic rectocele. Anatomic and subjective outcomes (vaginal bulge and defecatory) were collected 12 months postoperatively, including blinded Pelvic Organ Prolapse Quantification (POP-Q) examinations. Anatomic failure was defined as points Ap or Bp -1 or greater on POP-Q. Subjective failure was defined as no improvement or worsening of symptoms. We estimated number needed to treat and adjusted odds ratios (ORs). Assuming graft use is associated with 93% anatomic success, 63 women per group would be needed to detect a 20% difference at α=.05 and β=.20.
Results: One hundred sixty women were randomized; 137 had 12-month anatomic data (67 graft; 70 control). There was no difference in anatomic failure (12% compared with 9%, P=.5), vaginal bulge symptom failure (3% compared with 7%, P=.4, number needed to treat=26) or defecatory symptom failure (44% compared with 45%, P=.9, number needed to treat=91) for graft compared with control, respectively. Both groups reported improvement in vaginal bulge and defecatory symptoms (P<.05 for all). On multiple logistic regression, graft use was not associated with a decreased odds of anatomic failure (adjusted OR 1.36, 95% confidence interval [CI] 0.44-4.25), vaginal bulge symptoms (adjusted OR 0.46, 95% CI 0.08-2.68), or defecatory symptoms (adjusted OR 0.98, 95% CI 0.48-2.03).
Conclusion: Although rectocele repair by either approach is associated with improved symptoms, subintestinal submucosal graft augmentation was not superior to native tissue for anatomic or subjective outcomes at 12 months.
Clinical trial registration: ClinicalTrials.gov, www.clinicaltrials.gov, NCT00321867.
Conflict of interest statement
Financial Disclosure
The authors did not report any potential conflicts of interest.
Figures
References
-
- Sung VW, Rogers RG, Schaffer JI, et al. Graft use in transvaginal pelvic organ prolapse repair: a systematic review. Obstet Gynecol. 2008;112:1131–1142. - PubMed
-
- Rogers GR, Villarreal A, Kammerer-Doak D, Qualls C. Sexual function in women with and without urinary incontinence and/or pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2001;12:361–365. - PubMed
-
- Barber MD, Visco AG, Wyman JF, Fantl JA, Bump RC. Sexual function in women with urinary incontinence and pelvic organ prolapse. Obstet Gynecol. 2002;99:281–289. - PubMed
-
- Weber AM, Walters MD, Ballard LA, Booher DL, Piedmonte MR. Posterior vaginal prolapse and bowel function. Am J Obstet Gynecol. 1998;179:1446–1449. discussion 9–50. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
