

Prospective high-resolution respiratory-resolved whole-heart MRI for image-guided cardiovascular interventions
- PMID: 22183798
- PMCID: PMC3784045
- DOI: 10.1002/mrm.23216
Prospective high-resolution respiratory-resolved whole-heart MRI for image-guided cardiovascular interventions
Abstract
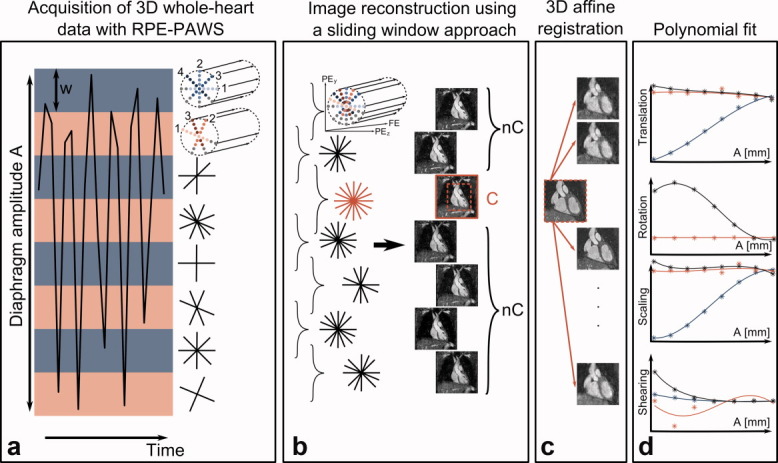
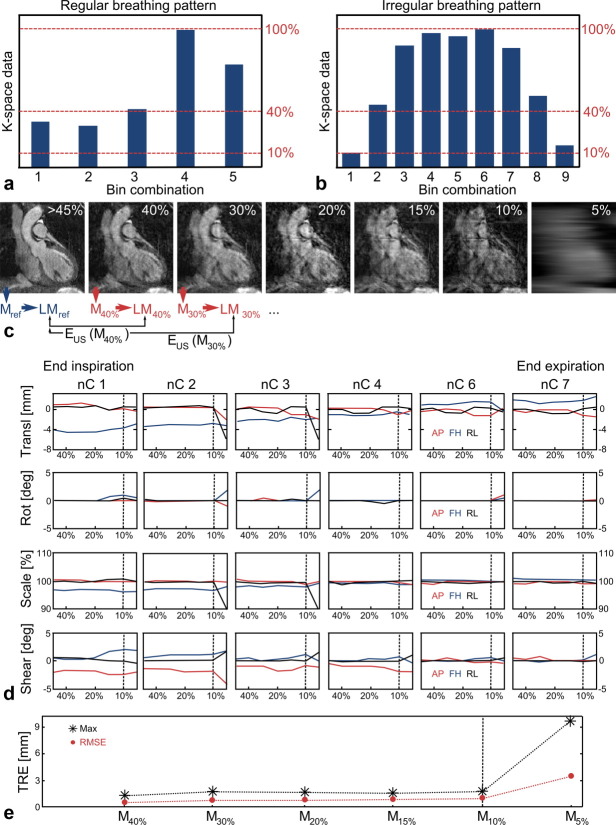
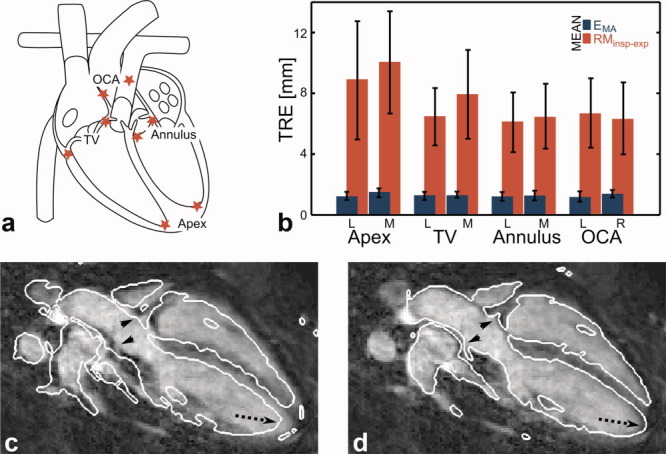
Cardiovascular diseases, including arrhythmias and heart failure, are commonly treated with percutaneous procedures guided by X-ray fluoroscopy. The visualization of the targeted structures can be enhanced using preacquired respiratory-resolved anatomic data (dynamic roadmap), which is displayed as an overlay onto X-ray fluoroscopy images. This article demonstrates how dynamic roadmaps using an affine motion model can be obtained from one respiratory-resolved three-dimensional whole-heart acquisition using the previously introduced Radial Phase Encoding-Phase Ordering with Automatic Window Selection method. Respiratory motion in different regions of the heart was analyzed in 10 volunteers, and it was shown that the use of dynamic roadmaps can reduce misalignment errors from more than 10 down to less than 1.5 mm. Furthermore, the results suggest that reliable motion information can be obtained from highly undersampled images due to the advantageous undersampling properties of the radial phase encoding trajectory. Finally, results of a three-dimensional dynamic roadmap obtained from a patient before catheter ablation for atrial fibrillation treatment are presented.
Copyright © 2011 Wiley Periodicals, Inc.
Figures

Similar articles
-
A subject-specific technique for respiratory motion correction in image-guided cardiac catheterisation procedures.Med Image Anal. 2009 Jun;13(3):419-31. doi: 10.1016/j.media.2009.01.003. Epub 2009 Jan 21. Med Image Anal. 2009. PMID: 19223220
-
3-D respiratory motion compensation during EP procedures by image-based 3-D lasso catheter model generation and tracking.Med Image Comput Comput Assist Interv. 2009;12(Pt 1):394-401. doi: 10.1007/978-3-642-04268-3_49. Med Image Comput Comput Assist Interv. 2009. PMID: 20426012
-
Respiratory motion compensation by model-based catheter tracking during EP procedures.Med Image Anal. 2010 Oct;14(5):695-706. doi: 10.1016/j.media.2010.05.006. Epub 2010 Jun 10. Med Image Anal. 2010. PMID: 20579931
-
[Three-dimensional reconstruction and remote navigation for catheter-guided atrial fibrillation ablation. Does it influence procedural outcomes?].Clin Res Cardiol Suppl. 2011 May;6:73-7. doi: 10.1007/s11789-011-0028-0. Clin Res Cardiol Suppl. 2011. PMID: 22528181 Review. German.
-
A review of 3D/2D registration methods for image-guided interventions.Med Image Anal. 2012 Apr;16(3):642-61. doi: 10.1016/j.media.2010.03.005. Epub 2010 Apr 13. Med Image Anal. 2012. PMID: 20452269 Review.
Cited by
-
Free-breathing 3D cardiac MRI using iterative image-based respiratory motion correction.Magn Reson Med. 2013 Oct;70(4):1005-15. doi: 10.1002/mrm.24538. Epub 2012 Nov 6. Magn Reson Med. 2013. PMID: 23132549 Free PMC article.
-
Three-dimensional heart locator and compressed sensing for whole-heart MR angiography.Magn Reson Med. 2016 May;75(5):2086-93. doi: 10.1002/mrm.25800. Epub 2015 Jun 10. Magn Reson Med. 2016. PMID: 26069182 Free PMC article.
-
Impact of cardiac and respiratory motion on the 3D accuracy of image-guided interventions on monoplane systems.Int J Comput Assist Radiol Surg. 2024 Feb;19(2):367-374. doi: 10.1007/s11548-023-02998-9. Epub 2023 Jul 21. Int J Comput Assist Radiol Surg. 2024. PMID: 37477817 Free PMC article.
-
Non-Cartesian parallel imaging reconstruction.J Magn Reson Imaging. 2014 Nov;40(5):1022-40. doi: 10.1002/jmri.24521. Epub 2014 Jan 10. J Magn Reson Imaging. 2014. PMID: 24408499 Free PMC article. Review.
References
-
- Razavi R, Mathuranu V, Hedge SR, Taylor AM. Clinical Cardiac MRI. Berlin, Heidelberg: Springer; 2005.
-
- Jordan PN, Christini DJ. Therapies for ventricular cardiac arrhythmias. Crit Rev Biomed Eng. 2005;33:557–604. - PubMed
-
- McGavigan AD, Kalman JM. Atrial anatomy and imaging in atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2006;17:S8–S15. - PubMed
-
- Dewire J, Calkins H. State-of-the-art and emerging technologies for atrial fibrillation ablation. Nat Rev Cardiol. 2010;7:129–138. - PubMed
-
- Duckett SG, Chiribiri A, Ginks MR, Sinclair S, Knowles BR, Botnar R, Carr-White GS, Rinaldi CA, Nagel E, Razavi R, Schaeffter T. Cardiac MRI to investigate myocardial scar and coronary venous anatomy using a slow infusion of dimeglumine gadobenate in patients undergoing assessment for cardiac resynchronization therapy. J Magn Reson Imaging. 2011;33:87–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
