

The cost-utility of adjuvant chemotherapy using docetaxel and cyclophosphamide compared with doxorubicin and cyclophosphamide in breast cancer
- PMID: 22184496
- PMCID: PMC3224037
- DOI: 10.3747/co.v18i6.810
The cost-utility of adjuvant chemotherapy using docetaxel and cyclophosphamide compared with doxorubicin and cyclophosphamide in breast cancer
Abstract
Purpose: The adoption of a chemotherapeutic regimen in oncologic practice is a function of both its clinical and its economic impacts on cancer management. For breast cancer, U.S. Oncology trial 9735 reported significant improvements in disease-free and overall survival favoring adjuvant tc (docetaxel 75 mg/m(2) and cyclophosphamide 600 mg/m(2) every 3 weeks for 4 cycles) compared with ac (doxorubicin 60 mg/ m(2) and cyclophosphamide 600 mg/m(2) every 3 weeks for 4 cycles). We carried out an economic evaluation to examine the cost-utility of adjuvant tc relative to ac, in terms of cost per quality-adjusted life year (qaly) gained, given the improved breast cancer outcomes and higher costs associated with the tc regimen.
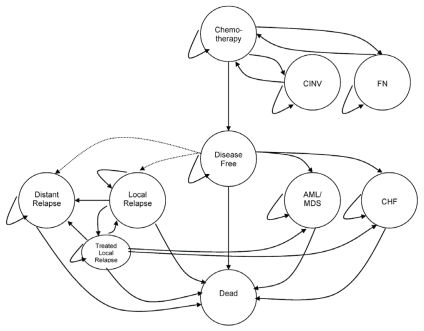
Methods: A Markov model was developed to calculate the cumulative costs and qalys gained over a 10-year horizon for hypothetical cohorts of women with breast cancer treated with ac or with tc. Event rates, costs, and utilities were derived from the literature and local resources. Efficacy and adverse events were based on results reported from U.S. Oncology trial 9735. The model takes a third-party direct payer perspective and reports its results in 2008 Canadian dollars. Costs and benefits were both discounted at 3%.
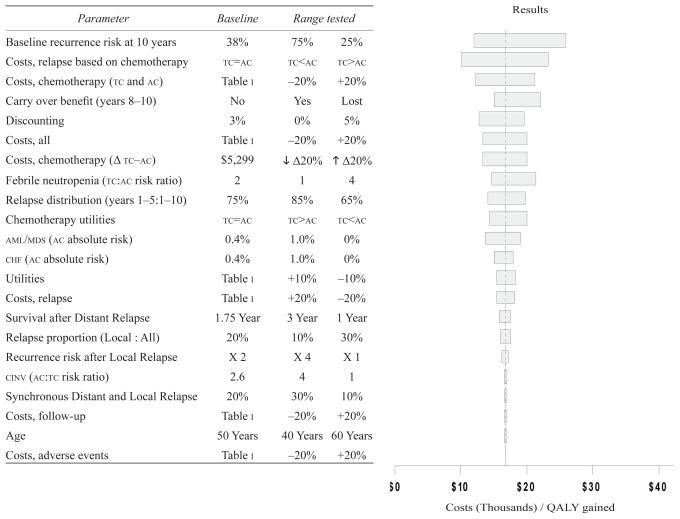
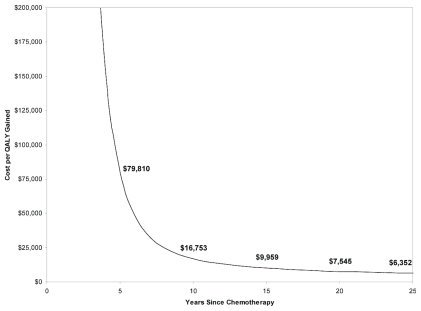
Results: At a 10-year horizon, tc was associated with $3,960 incremental costs and a 0.24 qaly gain compared with ac, for a favorable cost-utility of $16,753 per qaly gained. Results were robust to model assumptions and input parameters.
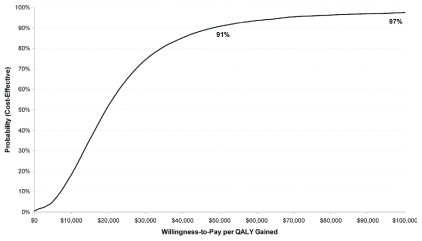
Conclusions: Relative to ac, tc is a cost-effective adjuvant chemotherapy regimen, with a cost-effectiveness ratio well below commonly applied thresholds.
Keywords: Breast cancer; ac chemotherapy, cost; adjuvant therapy; chemotherapy; tc chemotherapy; utility analysis.
Figures
Similar articles
-
Cost-effectiveness analysis of adjuvant therapy for operable breast cancer from a Chinese perspective: doxorubicin plus cyclophosphamide versus docetaxel plus cyclophosphamide.Pharmacoeconomics. 2009;27(10):873-86. doi: 10.2165/11314750-000000000-00000. Pharmacoeconomics. 2009. PMID: 19803541
-
Adjuvant chemotherapy for breast cancer: a cost-utility analysis of FEC-D vs. FEC 100.Breast Cancer Res Treat. 2008 Sep;111(2):261-7. doi: 10.1007/s10549-007-9770-x. Epub 2007 Oct 5. Breast Cancer Res Treat. 2008. PMID: 17914669
-
A Canadian economic analysis of U.S. Oncology Adjuvant Trial 9735.Curr Oncol. 2011 Apr;18(2):67-75. doi: 10.3747/co.v18i2.701. Curr Oncol. 2011. PMID: 21505597 Free PMC article.
-
Zoledronic acid: a pharmacoeconomic review of its use in the management of bone metastases.Pharmacoeconomics. 2008;26(3):251-68. doi: 10.2165/00019053-200826030-00007. Pharmacoeconomics. 2008. PMID: 18282018 Review.
-
[Cost-effectiveness of trastuzumab in the treatment of early stages breast cancer patients, in Portugal].Acta Med Port. 2010 May-Jun;23(3):475-82. Epub 2010 Jun 14. Acta Med Port. 2010. PMID: 20654267 Review. Portuguese.
Cited by
-
Cost-utility analysis of 21-gene assay for node-positive early breast cancer.Curr Oncol. 2019 Oct;26(5):307-318. doi: 10.3747/co.26.4769. Epub 2019 Oct 1. Curr Oncol. 2019. PMID: 31708649 Free PMC article.
-
Cost-Effectiveness Analysis for Therapy Sequence in Advanced Cancer: A Microsimulation Approach with Application to Metastatic Prostate Cancer.Med Decis Making. 2023 Oct-Nov;43(7-8):949-960. doi: 10.1177/0272989X231201621. Epub 2023 Oct 9. Med Decis Making. 2023. PMID: 37811793 Free PMC article.
-
Cost-Effectiveness of Neoadjuvant-Adjuvant Treatment Strategies for Women With ERBB2 (HER2)-Positive Breast Cancer.JAMA Netw Open. 2020 Nov 2;3(11):e2027074. doi: 10.1001/jamanetworkopen.2020.27074. JAMA Netw Open. 2020. PMID: 33226431 Free PMC article. Clinical Trial.
-
The cost-effectiveness of neoadjuvant chemotherapy in women with locally advanced breast cancer: Adriamycin and cyclophosphamide in comparison with paclitaxel and gemcitabine.J Res Med Sci. 2018 Jun 6;23:57. doi: 10.4103/jrms.JRMS_644_17. eCollection 2018. J Res Med Sci. 2018. PMID: 30057641 Free PMC article.
-
Disparities in Breast Cancer: Private Patients Have Better Outcomes Than Public Patients.World J Surg. 2018 Mar;42(3):727-735. doi: 10.1007/s00268-017-4187-0. World J Surg. 2018. PMID: 28819769
References
-
- National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Ver. 2.2011. Fort Washington, PA: NCCN; [cited October 21, 2011]. [Available online at: http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf; (no-cost registration required)
LinkOut - more resources
Full Text Sources
Other Literature Sources
