

Efficient practices associated with diagnosis, treatment and management of fibromyalgia among primary care physicians
- PMID: 22184554
- PMCID: PMC3298044
- DOI: 10.1155/2011/367059
Efficient practices associated with diagnosis, treatment and management of fibromyalgia among primary care physicians
Abstract
Objectives: To describe beliefs and practice patterns of primary care physicians (PCPs) providing fibromyalgia (FM) care, and to characterize differences between PCPs who report being able to provide timely and beneficial care versus the remaining PCPs.
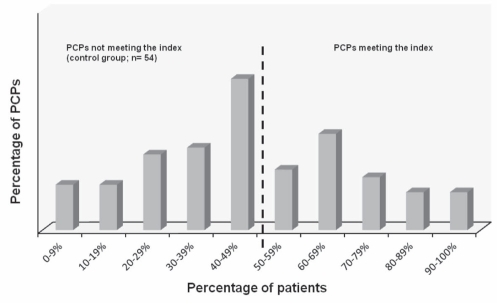
Methods: A mixed-methods approach including surveys followed by semi-structured focus groups among United States-based PCPs in seven cities was used. Post hoc, a composite threshold of timely and beneficial care, defined as PCPs reports of at least one-half of their patients achieving an 'acceptable' quality of life within one to four office visits after diagnosis, was created to compare subgroups.
Results: Forty-six per cent of PCPs reported some uncertainty when diagnosing FM. PCPs reported personally treating approximately two-thirds of their patients (63%), and reported an average of three dosage titrations. In a post hoc exploratory analysis, 42.5% of PCPs met a composite threshold of self-reported timely and beneficial FM care. These PCPs reported fewer office visits to confirm an FM diagnosis (2.7 versus 4.0 visits [P<0.01]) and more patients with 'significant improvement' (38% versus 23% [P<0.01]) after six months of treatment compared with the remaining PCPs.
Conclusions: Physicians self-reported an inadequacy in diagnosing, treating and managing patients with FM in current practice. A subset of PCPs, however, perceived an ability to reach a definitive diagnosis and initiate treatment plans relatively sooner than the other respondents. If the perception of this subset can be confirmed with objective clinical outcomes, and these behaviours modelled, steps could be taken to improve FM care within the broader PCP setting.
OBJECTIFS :: Décrire les croyances et les profils de pratique des médecins de première ligne (MPL) qui fournissent des soins en fibromyalgie (FM) et caractériser les différences entre les MPL qui déclarent pouvoir fournir des soins rapides et bénéfiques et les autres MPL.
MÉTHODOLOGIE :: Les chercheurs ont adopté une méthodologie mixte incluant des sondages suivis de groupes de travail semi-structurés chez des MPL provenant de sept villes des États-Unis. Pour comparer les sous-groupes, ils ont ensuite créé un seuil composite de soins rapides et bénéfiques, définis comme la déclaration des MPL indiquant qu’au moins la moitié de leurs patients étaient parvenus à une qualité de vie « acceptable » au bout de une à quatre visites en cabinet après le diagnostic.
RÉSULTATS :: Quarante-six pour cent des MPL ont déclaré une certaine incertitude lorsqu’ils diagnostiquent une FM. Les MPL ont déclaré traiter personnellement environ les deux tiers de leurs patients (63 %) et effectuer une moyenne de trois titrages de posologie. Dans une analyse exploratoire a posteriori, 42,5 % des MPL ont respecté un seuil composite de soins rapides et bénéfiques de la FM. Ces MPL ont déclaré moins de visites en cabinet pour confirmer un diagnostic de FM (2,7 par rapport à 4,0 [P<0,01]) et plus de patients qui présentaient une « amélioration importante » (38 % par rapport à 23 % [P<0,01]) six mois après le traitement par rapport aux autres MPL.
CONCLUSIONS :: Les médecins ont eux-mêmes déclaré une incapacité à diagnostiquer, à traiter et à prendre en charge les patients ayant une FM dans leur pratique. Un sous-groupe de MPL a toutefois perçu une capacité de parvenir à un diagnostic définitif et à amorcer un plan thérapeutique relativement plus vite que les autres répondants. Si la perception de ce sous-groupe peut être confirmée par des issues cliniques objectives et si ces comportements peuvent être transformés en modèles, on pourra prendre des mesures pour améliorer les soins de la FM par l’ensemble des MPL.
Figures
Similar articles
-
The impact of 'best-practice' patient care in fibromyalgia on practice economics.J Eval Clin Pract. 2012 Aug;18(4):793-8. doi: 10.1111/j.1365-2753.2011.01678.x. Epub 2011 May 3. J Eval Clin Pract. 2012. PMID: 21539697
-
A patient and physician survey of fibromyalgia across Latin America and Europe.BMC Musculoskelet Disord. 2013 Jun 14;14:188. doi: 10.1186/1471-2474-14-188. BMC Musculoskelet Disord. 2013. PMID: 23767857 Free PMC article.
-
Survey of physician experiences and perceptions about the diagnosis and treatment of fibromyalgia.BMC Health Serv Res. 2012 Oct 10;12:356. doi: 10.1186/1472-6963-12-356. BMC Health Serv Res. 2012. PMID: 23051101 Free PMC article.
-
Office management of fibromyalgia.Rheum Dis Clin North Am. 2002 May;28(2):437-46, xi. doi: 10.1016/s0889-857x(01)00008-4. Rheum Dis Clin North Am. 2002. PMID: 12122929 Review.
-
Improving the recognition and diagnosis of fibromyalgia.Mayo Clin Proc. 2011 May;86(5):457-64. doi: 10.4065/mcp.2010.0738. Mayo Clin Proc. 2011. PMID: 21531887 Free PMC article. Review.
Cited by
-
Diagnostic difficulty, delayed diagnosis, and increased tendencies of surgical treatment in fibromyalgia syndrome.Clin Rheumatol. 2022 Mar;41(3):831-837. doi: 10.1007/s10067-021-05970-7. Epub 2021 Oct 21. Clin Rheumatol. 2022. PMID: 34671855
-
Perspectives on Living With Fibromyalgia.Glob Qual Nurs Res. 2016 Jul 6;3:2333393616658141. doi: 10.1177/2333393616658141. eCollection 2016 Jan-Dec. Glob Qual Nurs Res. 2016. PMID: 28620627 Free PMC article.
-
Quality of rheumatology care for patients with fibromyalgia and chronic pain syndromes.BMJ Open Qual. 2021 Mar;10(1):e001061. doi: 10.1136/bmjoq-2020-001061. BMJ Open Qual. 2021. PMID: 33766832 Free PMC article.
-
Implication of the Nociplastic Features for Clinical Diagnosis of Fibromyalgia: Development of the Preliminary Nociplastic-Based Fibromyalgia Features (NFF) Tool.ACR Open Rheumatol. 2022 Mar;4(3):260-268. doi: 10.1002/acr2.11390. Epub 2021 Dec 22. ACR Open Rheumatol. 2022. PMID: 34936234 Free PMC article.
-
Fibromyalgia: management strategies for primary care providers.Int J Clin Pract. 2016 Feb;70(2):99-112. doi: 10.1111/ijcp.12757. Int J Clin Pract. 2016. PMID: 26817567 Free PMC article. Review.
References
-
- Perrot S, Dickenson AH, Bennett RM. Fibromyalgia: Harmonizing science with clinical practice considerations. Pain Pract. 2008;8:177–89. - PubMed
-
- Peterson EL. Fibromyalgia – management of a misunderstood disorder. J Am Acad Nurse Pract. 2007;19:341–8. - PubMed
-
- Silverman S, Brandenberg N, Mucha L. Costs and utilization of pharmacologic interventions for fibromyalgia and its comorbidities (Poster 285). American Pain Society Annual Meeting; Tampa. May 8 to 10, 2008.
-
- Rothenberg R. Fibromyalgia: documentation & treatment: A guide for primary care professionals. Fibromyalgia Frontiers. 2007;15:1–6.
-
- Neumann L, Buskila D. Epidemiology of fibromyalgia. Curr Pain Headache Rep. 2003;7:362–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
