

Bony metastases: assessing response to therapy with whole-body diffusion MRI
- PMID: 22185786
- PMCID: PMC3266569
- DOI: 10.1102/1470-7330.2011.9034
Bony metastases: assessing response to therapy with whole-body diffusion MRI
Abstract
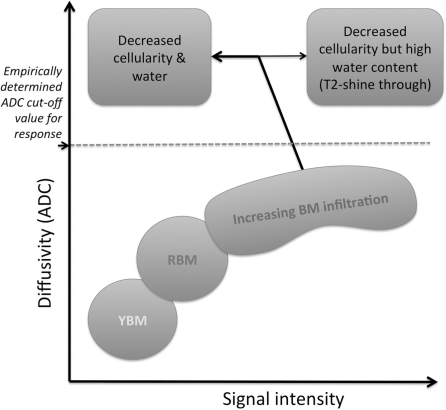
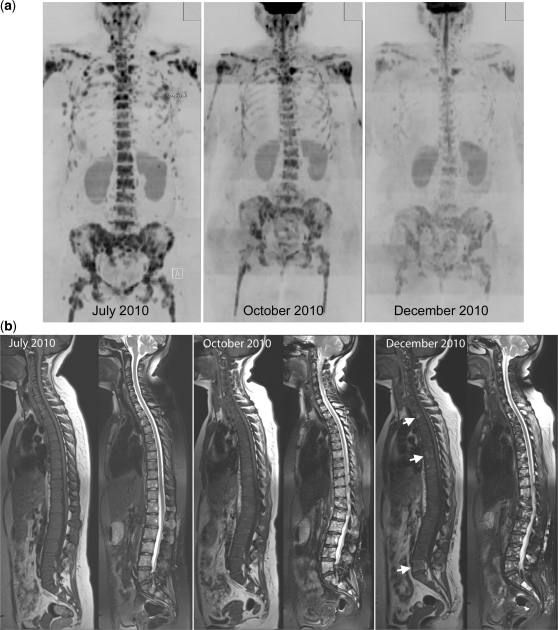
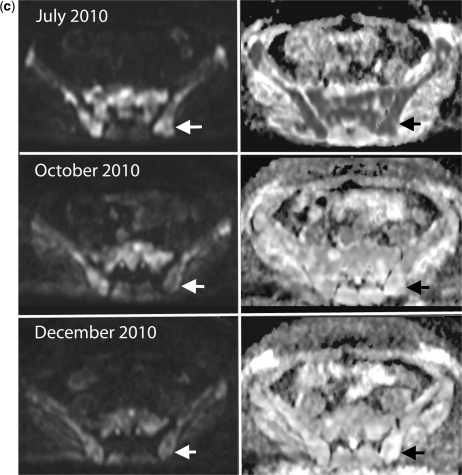
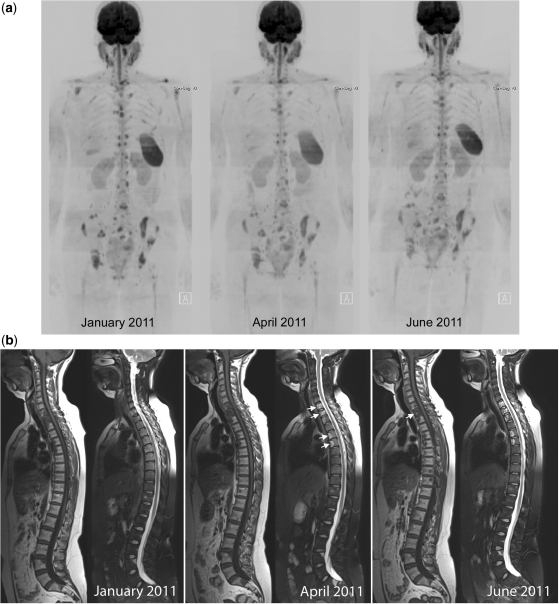
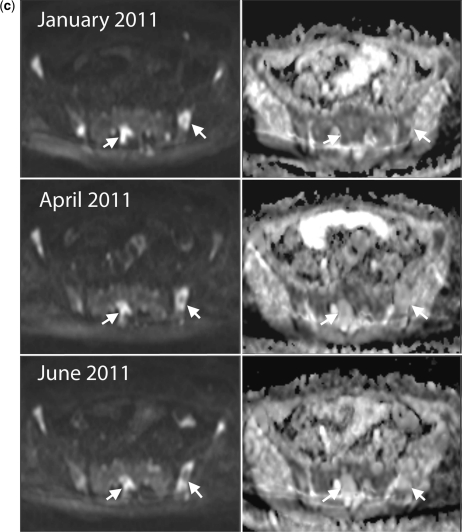
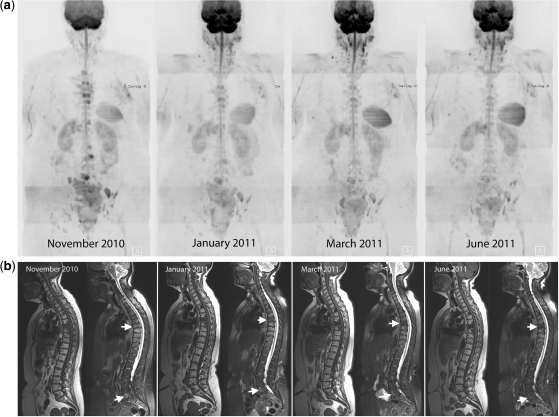
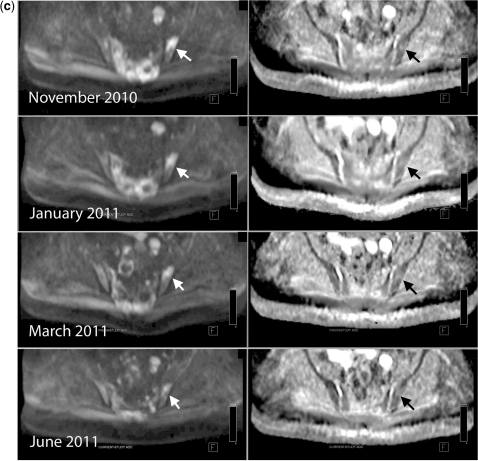
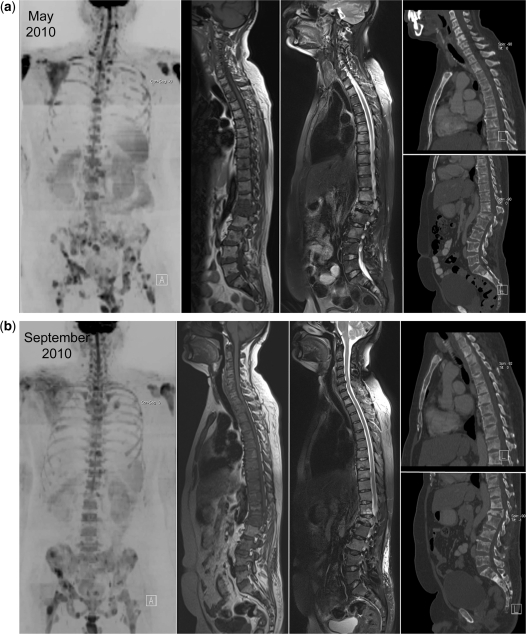
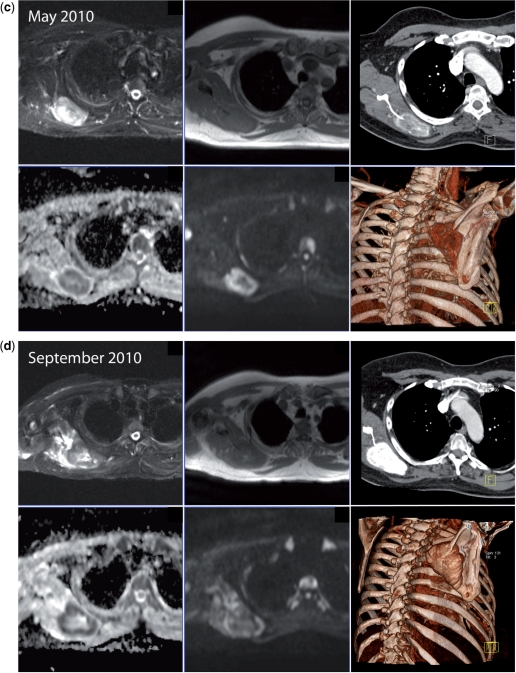
There are no universally accepted methods for assessing tumour response in skeletal sites with metastatic disease; response is assessed by a combination of imaging tests, serum and urine biochemical markers and symptoms assessments. Whole-body diffusion magnetic resonance imaging excels at bone marrow assessments at diagnosis and for therapy evaluations. It can potentially address unmet clinical and pharmaceutical needs for a reliable measure of tumour response. Signal intensity on high b-value images and apparent diffusion coefficient values can be related to underlying biophysical properties of skeletal metastases. Four patterns of change in response to therapy are described this review. Therapy response criteria need to be tested in prospective clinical studies that incorporate conventional measures of patient benefit.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical