

Rural and urban differences in metabolic profiles in a Cameroonian population
- PMID: 22187583
- PMCID: PMC3282926
- DOI: 10.4314/pamj.v10i0.72204
Rural and urban differences in metabolic profiles in a Cameroonian population
Abstract
Introduction: The difference between modern lifestyle in urban areas and the traditional way of life in rural areas may affect the population's health in developing countries proportionally. In this study, we sought to describe and compare the metabolic (fasting blood sugar and lipid profile) profile in an urban and rural sample of a Cameroonian population, and study the association to anthropometric risk factors of obesity.
Methods: 332 urban and 120 rural men and women originating from the Sanaga Maritime Department and living in the Littoral Region in Cameroon voluntarily participated in this study. In all participants, measurement of height, weight, waist circumference, hip circumference, blood pressure systolic (SBP) and blood pressure diastolic (DBP), resting heart rate (RHR), blood glucose and lipids was carried out using standard methods. Total body fat (BF%) was measured using bio-impedancemetry. Body mass index (BMI) and waist to hip ratio (WHR) were calculated. Low Density Lipoprotein-cholesterol (LDL-c) concentrations were calculated using the Friedwald formula. World Health Organization criteria were used to define high and low levels of blood pressure, metabolic and anthropometric factors.
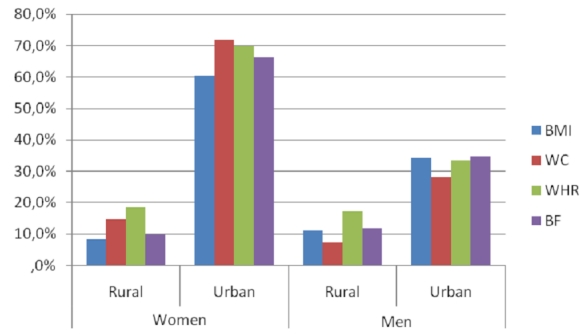
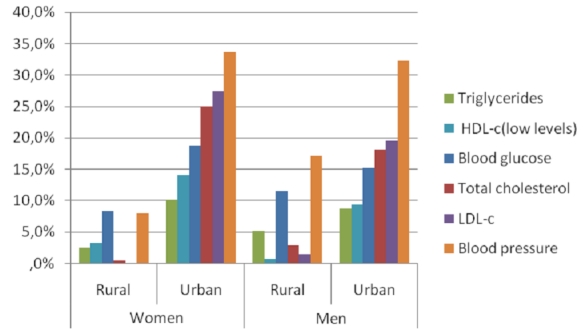
Results: The highest blood pressure values were found in rural men. Concerning resting heart rate, only the youngest women's age group showed a significant difference between urban and rural areas (79 ± 14 bpm vs 88 ± 12 bpm, p = 0.04) respectively. As opposed to the general tendency in our population, blood glucose was higher in rural men and women compared to their urban counterparts in the older age group (6.00 ± 2.56 mmol/L vs 5.72 ± 2.72 mmol/L, p = 0.030; 5.77 ± 3.72 vs 5.08 ± 0.60, p = 0,887 respectively). Triglycerides (TG) were significantly higher in urban than rural men (1.23 ± 0.39 mmol/L vs 1.17 ± 0.64 mmol/L, p = 0.017). High Density Lipoprotein-cholesterol (HDL-c) levels were higher in rural compared to urban men (2.60 ± 0.10 35mmol/L vs 1.97 ± 1.14 mmol/L, p<0.001 respectively). However, total Cholesterol (TC) and LDL-c were significantly higher in urban than in rural men (p<0.001 and p = 0.005) and women (p<0.001 respectively. Diabetes' rate in this population was 6.6%. This rate was higher in the rural (8.3%) than in the urban area (6.0%). Age and RHR were significantly higher in diabetic women than in non-diabetics (p = 0.007; p = 0.032 respectively). In a multiple regression, age was an independent predictor of SBP, DBP and RHR in the entire population. Age predicted blood glucose in rural women only. BMI, WC and BF% were independent predictors of RHR in rural population, especially in men. WC and BF% predicted DBP in rural men only. Anthropometric parameters did not predict the lipid profile.
Conclusion: Lipid profile was less atherogenic in rural than in urban area. The rural population was older than the urban one. Blood pressure and blood glucose were positively associated to age in men and women respectively; this could explain the higher prevalence of diabetes in rural than in urban area. The association of these metabolic variables to obesity indices is more frequent and important in urban than in rural area.
Figures
Similar articles
-
Waist circumference and obesity-related abnormalities in French and Cameroonian adults: the role of urbanization and ethnicity.Int J Obes (Lond). 2010 Mar;34(3):446-53. doi: 10.1038/ijo.2009.256. Epub 2010 Jan 12. Int J Obes (Lond). 2010. PMID: 20065972 Free PMC article.
-
Obesity and lipid profiles in middle aged men and women in Tanzania.East Afr Med J. 2002 Feb;79(2):58-64. doi: 10.4314/eamj.v79i2.8901. East Afr Med J. 2002. PMID: 12380877
-
Lipoprotein lipids and the prevalence of hyperlipidaemia in rural India.J Cardiovasc Risk. 1994 Aug;1(2):179-84. doi: 10.1177/174182679400100213. J Cardiovasc Risk. 1994. PMID: 7606632
-
[Lipid profile comparison between pre- and post-menopausal women].Zhonghua Xin Xue Guan Bing Za Zhi. 2016 Sep 24;44(9):799-804. doi: 10.3760/cma.j.issn.0253-3758.2016.09.013. Zhonghua Xin Xue Guan Bing Za Zhi. 2016. PMID: 27667280 Chinese.
-
Beyond Boundaries: A Comprehensive Review of Anthropometric Indices in Urban and Rural India.Cureus. 2024 Feb 9;16(2):e53944. doi: 10.7759/cureus.53944. eCollection 2024 Feb. Cureus. 2024. PMID: 38468989 Free PMC article. Review.
Cited by
-
Prevalence of metabolic syndrome and components in rural, semi-urban and urban areas in the littoral region in Cameroon: impact of physical activity.J Health Popul Nutr. 2023 Sep 11;42(1):95. doi: 10.1186/s41043-023-00415-0. J Health Popul Nutr. 2023. PMID: 37697395 Free PMC article.
-
Intake of foods high in saturated fats, vegetarian dietary pattern, and sociodemographic characteristics associated with body weight in Peruvian university students.Front Nutr. 2024 Mar 20;11:1361091. doi: 10.3389/fnut.2024.1361091. eCollection 2024. Front Nutr. 2024. PMID: 38571749 Free PMC article.
-
Characteristics of participants who take up screening tests for diabetes and lipid disorders: a systematic review.BMJ Open. 2022 Apr 29;12(4):e055764. doi: 10.1136/bmjopen-2021-055764. BMJ Open. 2022. PMID: 35487721 Free PMC article.
-
The lipid profile of HIV-infected patients receiving antiretroviral therapy in a rural Cameroonian population.BMC Public Health. 2014 Mar 7;14:236. doi: 10.1186/1471-2458-14-236. BMC Public Health. 2014. PMID: 24606888 Free PMC article.
-
Body composition and physical activity as mediators in the relationship between socioeconomic status and blood pressure in young South African women: a structural equation model analysis.BMJ Open. 2018 Dec 19;8(12):e023404. doi: 10.1136/bmjopen-2018-023404. BMJ Open. 2018. PMID: 30573484 Free PMC article.
References
-
- Rosenbaum Michael, Leibel Rudolph L. The Physiology of Body Weight Regulation: Relevance to the Etiology of Obesity in Children. Pediatrics. 1998;101:525–39. - PubMed
-
- Misra A, Khurana L. Obesity and the Metabolic Syndrome in developing countries. J Clin Endocrinol Metab. 2008 Nov;93(11 Suppl 1):S9–30. - PubMed
-
- Guthold R, Ono T, Strong KL, et al. Worldwide variability in physical inactivity a 51-country survey. Am J Prev Med. 2008 Jun;34(6):486–94. - PubMed
-
- Buysschaert M. L'obésité de la physiopathologie au traitement. Louvain med. 2001;120:S63–S66. 2001.
-
- Popkin BM. Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases. Am J Clin Nutr. 2006 Aug;84(2):289–98. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
