

Tension of knotted surgical sutures shows tissue specific rapid loss in a rodent model
- PMID: 22188826
- PMCID: PMC3275509
- DOI: 10.1186/1471-2482-11-36
Tension of knotted surgical sutures shows tissue specific rapid loss in a rodent model
Abstract
Background: Every surgical suture compresses the enclosed tissue with a tension that depends from the knotting force and the resistance of the tissue. The aim of this study was to identify the dynamic change of applied suture tension with regard to the tissue specific cutting reaction.
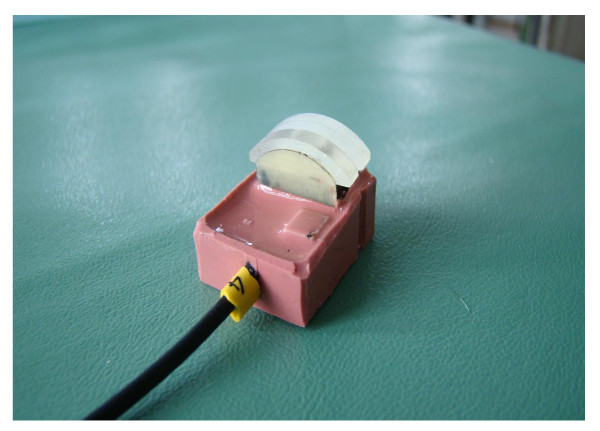
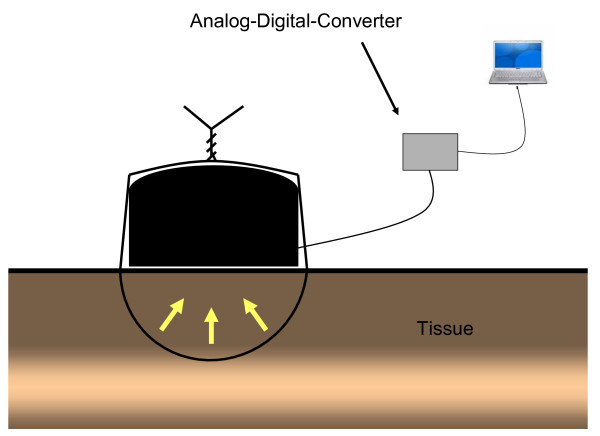
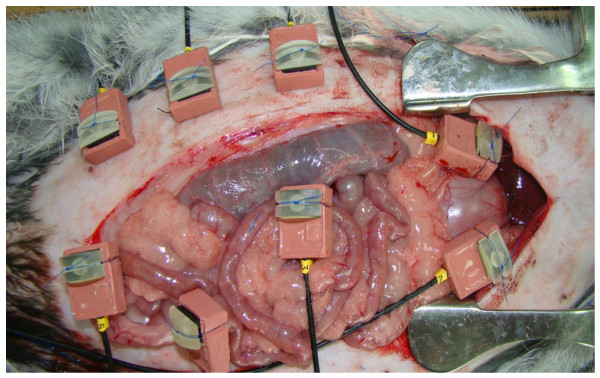
Methods: In rabbits we placed single polypropylene sutures (3/0) in skin, muscle, liver, stomach and small intestine. Six measurements for each single organ were determined by tension sensors for 60 minutes. We collected tissue specimens to analyse the connective tissue stability by measuring the collagen/protein content.
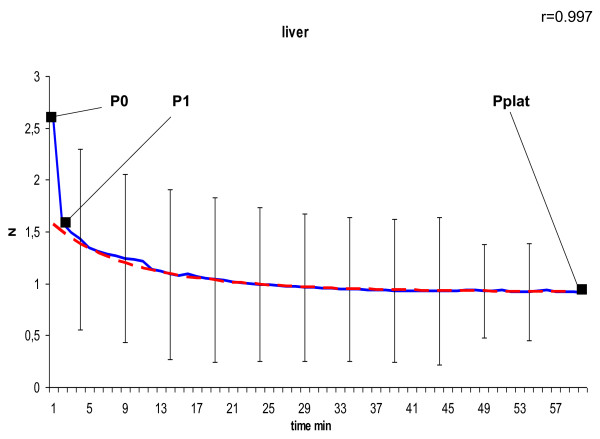
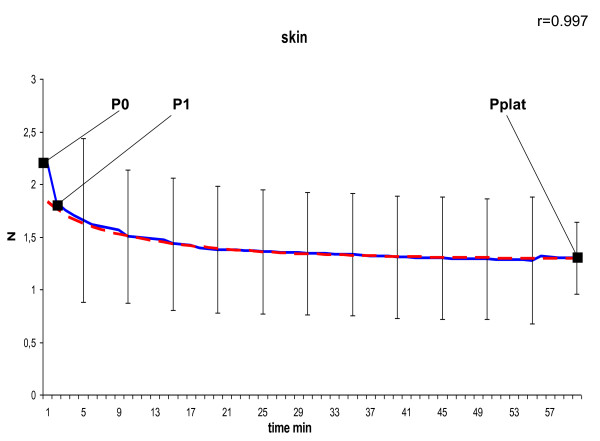
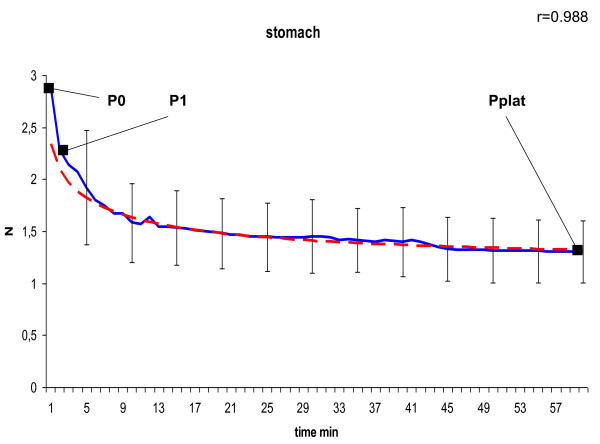
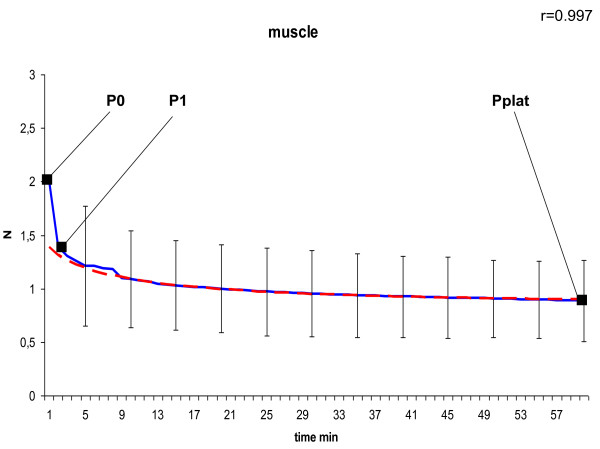
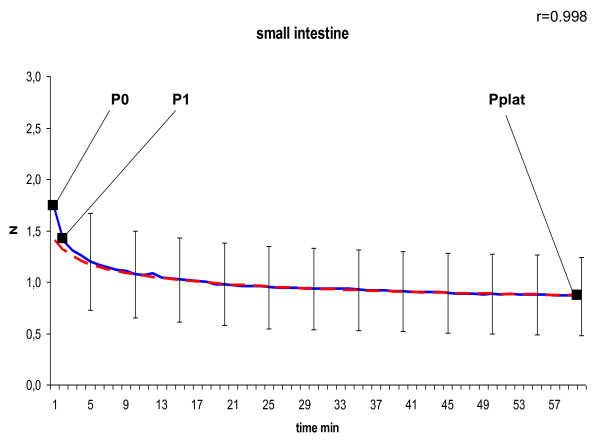
Results: We identified three phases in the process of suture loosening. The initial rapid loss of the first phase lasts only one minute. It can be regarded as cutting through damage of the tissue. The percentage of lost tension is closely related to the collagen content of the tissue (r = -0.424; p = 0.016). The second phase is characterized by a slower decrease of suture tension, reflecting a tissue specific plastic deformation. Phase 3 is characterized by a plateau representing the remaining structural stability of the tissue. The ratio of remaining tension to initial tension of phase 1 is closely related to the collagen content of the tissue (r = 0.392; p = 0.026).
Conclusions: Knotted non-elastic monofilament sutures rapidly loose tension. The initial phase of high tension may be narrowed by reduction of the surgeons' initial force of the sutures' elasticity to those of the tissue. Further studies have to confirm, whether reduced tissue compression and less local damage permits improved wound healing.
Figures
Similar articles
-
New suture materials for midline laparotomy closure: an experimental study.BMC Surg. 2014 Sep 17;14:70. doi: 10.1186/1471-2482-14-70. BMC Surg. 2014. PMID: 25231161 Free PMC article.
-
Torsion of monofilament and polyfilament sutures under tension decreases suture strength and increases risk of suture fracture.J Mech Behav Biomed Mater. 2012 Aug;12:168-73. doi: 10.1016/j.jmbbm.2012.02.001. Epub 2012 Feb 23. J Mech Behav Biomed Mater. 2012. PMID: 22762905
-
The Surgical Suture.Aesthet Surg J. 2019 Mar 14;39(Suppl_2):S67-S72. doi: 10.1093/asj/sjz036. Aesthet Surg J. 2019. PMID: 30869751
-
Prevention of incisional hernias: how to close a midline incision.Surg Clin North Am. 2013 Oct;93(5):1027-40. doi: 10.1016/j.suc.2013.06.009. Surg Clin North Am. 2013. PMID: 24035074 Review.
-
Suture choice and other methods of skin closure.Surg Clin North Am. 2009 Jun;89(3):627-41. doi: 10.1016/j.suc.2009.03.001. Surg Clin North Am. 2009. PMID: 19465201 Review.
Cited by
-
Developing and validating an implantable suture tension sensor.Heliyon. 2024 Apr 3;10(8):e28907. doi: 10.1016/j.heliyon.2024.e28907. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38660291 Free PMC article.
-
Development of incisional herniation after midline laparotomy.BJS Open. 2017 May 10;1(1):18-23. doi: 10.1002/bjs5.3. eCollection 2017 Feb. BJS Open. 2017. PMID: 29951601 Free PMC article.
-
The Best Closure Technique Without Mesh in Elective Midline Laparotomy Closure.J Abdom Wall Surg. 2022 Dec 7;1:10962. doi: 10.3389/jaws.2022.10962. eCollection 2022. J Abdom Wall Surg. 2022. PMID: 38314158 Free PMC article. Review.
-
Quantifying fascial tension in ventral hernia repair and component separation.Hernia. 2021 Feb;25(1):107-114. doi: 10.1007/s10029-020-02268-6. Epub 2020 Jul 27. Hernia. 2021. PMID: 32719913
-
Early Experience with Mesh Suture for DIEP Flap Abdominal Site Closures.Plast Reconstr Surg Glob Open. 2024 Aug 22;12(8):e6095. doi: 10.1097/GOX.0000000000006095. eCollection 2024 Aug. Plast Reconstr Surg Glob Open. 2024. PMID: 39175518 Free PMC article.
References
-
- Ratner D, Nelson BR, Johnson TM. Basic suture materials and suturing techniques. Semin Dermatol. 1994;13:20–26. - PubMed
-
- Seiler CM, Bruckner T, Diener MK, Papyan A, Golcher H, Seidlmayer C. et al.Interrupted or continuous slowly absorbable sutures for closure of primary elective midline abdominal incisions: a multicenter randomized trial (INSECT: ISRCTN24023541) 1. Ann Surg. 2009;249:576–582. doi: 10.1097/SLA.0b013e31819ec6c8. - DOI - PubMed
-
- Hogstrom H, Haglund U, Zederfeldt B. Suture technique and early breaking strength of intestinal anastomoses and laparotomy wounds 4. Acta Chir Scand. 1985;151:441–443. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
