

Prediction of new clinical vertebral fractures in elderly men using finite element analysis of CT scans
- PMID: 22190331
- PMCID: PMC3510751
- DOI: 10.1002/jbmr.1539
Prediction of new clinical vertebral fractures in elderly men using finite element analysis of CT scans
Abstract
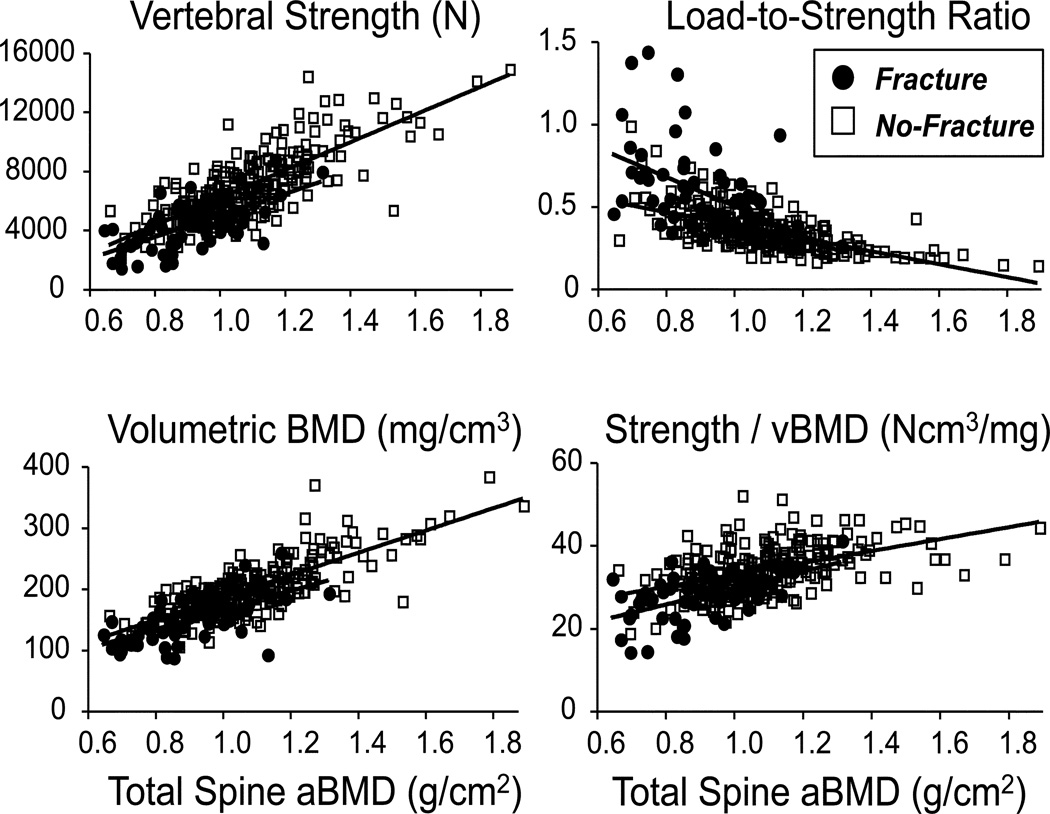
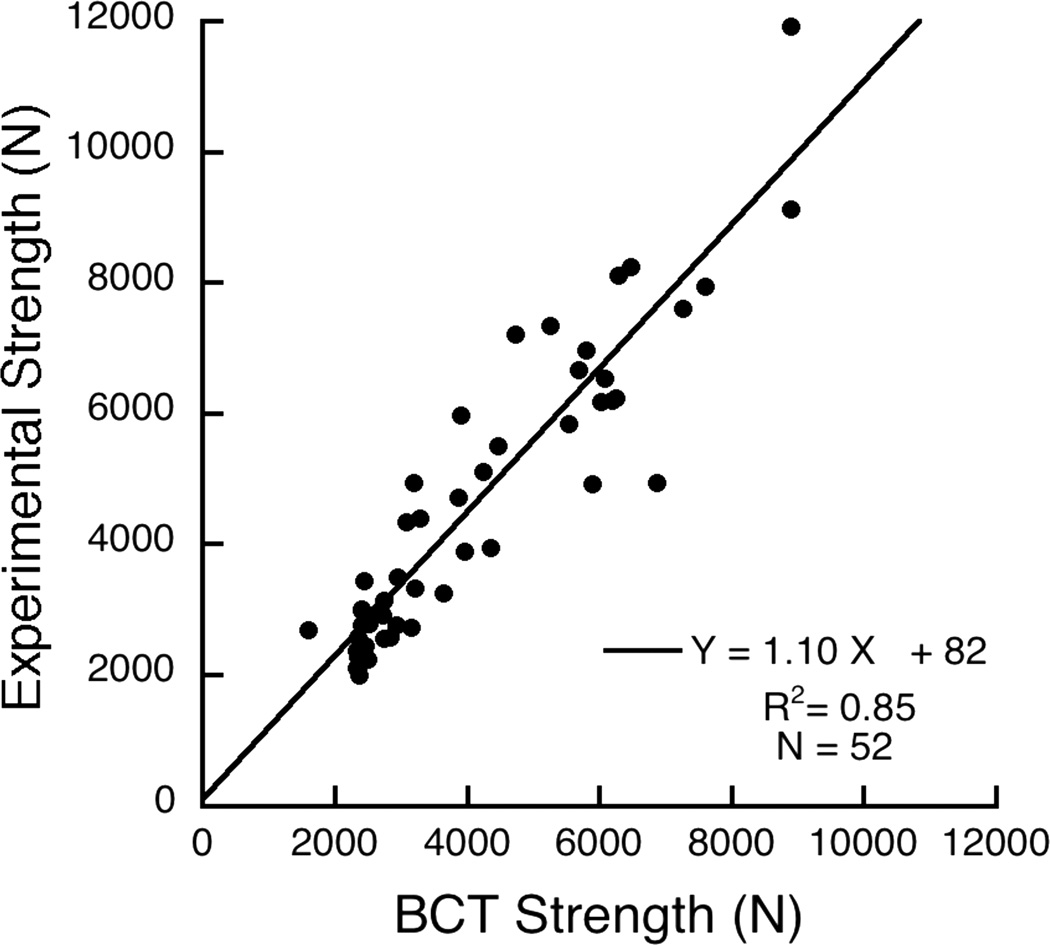
Vertebral strength, as estimated by finite element analysis of computed tomography (CT) scans, has not yet been compared against areal bone mineral density (BMD) by dual-energy X-ray absorptiometry (DXA) for prospectively assessing the risk of new clinical vertebral fractures. To do so, we conducted a case-cohort analysis of 306 men aged 65 years and older, which included 63 men who developed new clinically-identified vertebral fractures and 243 men who did not, all observed over an average of 6.5 years. Nonlinear finite element analysis was performed on the baseline CT scans, blinded to fracture status, to estimate L1 vertebral compressive strength and a load-to-strength ratio. Volumetric BMD by quantitative CT and areal BMD by DXA were also evaluated. We found that, for the risk of new clinical vertebral fracture, the age-adjusted hazard ratio per standard deviation change for areal BMD (3.2; 95% confidence interval [CI], 2.0-5.2) was significantly lower (p < 0.005) than for strength (7.2; 95% CI, 3.6-14.1), numerically lower than for volumetric BMD (5.7; 95% CI, 3.1-10.3), and similar for the load-to-strength ratio (3.0; 95% CI, 2.1-4.3). After also adjusting for race, body mass index (BMI), clinical center, and areal BMD, all these hazard ratios remained highly statistically significant, particularly those for strength (8.5; 95% CI, 3.6-20.1) and volumetric BMD (9.4; 95% CI, 4.1-21.6). The area-under-the-curve for areal BMD (AUC = 0.76) was significantly lower than for strength (AUC = 0.83, p = 0.02), volumetric BMD (AUC = 0.82, p = 0.05), and the load-to-strength ratio (AUC = 0.82, p = 0.05). We conclude that, compared to areal BMD by DXA, vertebral compressive strength and volumetric BMD consistently improved vertebral fracture risk assessment in this cohort of elderly men.
Copyright © 2012 American Society for Bone and Mineral Research.
Conflict of interest statement
The funding agencies had no role in the design and conduct of the study, in the collection, management, analysis, and interpretation of the data, or in the preparation, review, or approval of the manuscript. Dr. Keaveny has a financial interest in O.N. Diagnostics and both he and the company may benefit from the results of this work. All other authors state that they have no conflict of interest.
Figures
References
-
- Black DM, Arden NK, Palermo L, Pearson J, Cummings SR. Prevalent vertebral deformities predict hip fractures and new vertebral deformities but not wrist fractures. Study of Osteoporotic Fractures Research Group. J Bone Miner Res. 1999;14:821–828. - PubMed
-
- Cummings SR, Bates D, Black DM. Clinical use of bone densitometry - Scientific review. J Am Med Assoc. 2002;288:1889–1897. - PubMed
-
- Schuit SC, van der Klift M, Weel AE, de Laet CE, Burger H, Seeman E, Hofman A, Uitterlinden AG, van Leeuwen JP, Pols HA. Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam Study. Bone. 2004;34:195–202. - PubMed
-
- Siris ES, Chen YT, Abbott TA, Barrett-Connor E, Miller PD, Wehren LE, Berger ML. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med. 2004;164:1108–1112. - PubMed
-
- Liebschner MA, Kopperdahl DL, Rosenberg WS, Keaveny TM. Finite element modeling of the human thoracolumbar spine. Spine. 2003;28:559–565. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AR45632/AR/NIAMS NIH HHS/United States
- R01 AR049828/AR/NIAMS NIH HHS/United States
- U01 AR45647/AR/NIAMS NIH HHS/United States
- U01 AR052234/AR/NIAMS NIH HHS/United States
- U01 AR45614/AR/NIAMS NIH HHS/United States
- U01 AR045654/AR/NIAMS NIH HHS/United States
- R01 AR043784/AR/NIAMS NIH HHS/United States
- U01-AG027810/AG/NIA NIH HHS/United States
- U01 AR045583/AR/NIAMS NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- R44 AR052234/AR/NIAMS NIH HHS/United States
- U01 AR045614/AR/NIAMS NIH HHS/United States
- U01 AR45654/AR/NIAMS NIH HHS/United States
- U01 AR45583/AR/NIAMS NIH HHS/United States
- AR49828/AR/NIAMS NIH HHS/United States
- R43 AR052234/AR/NIAMS NIH HHS/United States
- U01 AR045647/AR/NIAMS NIH HHS/United States
- U01 AR45580/AR/NIAMS NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- UL1 RR024140/RR/NCRR NIH HHS/United States
- U01 AR045580/AR/NIAMS NIH HHS/United States
- AR43784/AR/NIAMS NIH HHS/United States
- U01 AG18197/AG/NIA NIH HHS/United States
- U01 AG018197/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- U01 AR045632/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
