

Intrauterine growth retardation and nonalcoholic Fatty liver disease in children
- PMID: 22190925
- PMCID: PMC3235463
- DOI: 10.1155/2011/269853
Intrauterine growth retardation and nonalcoholic Fatty liver disease in children
Abstract
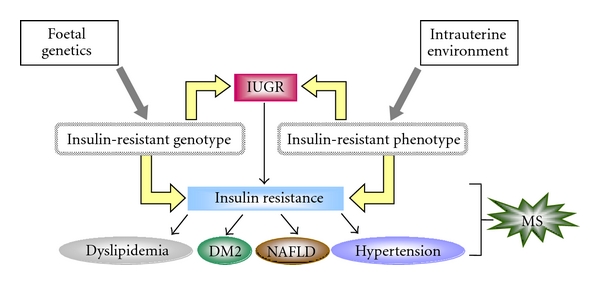
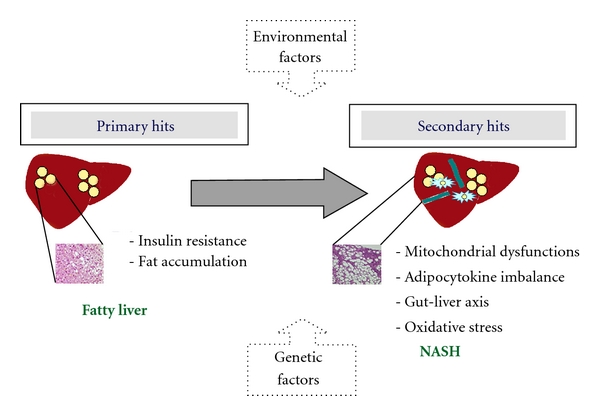
Intrauterine growth retardation (IUGR), the most important cause of perinatal mortality and morbidity, is defined as a foetal growth less than normal for the population, often used as synonym of small for gestational age (SGA). Studies demonstrated the relationships between metabolic syndrome (MS) and birthweight. This study suggested that, in children, adolescents, and adults born SGA, insulin resistance could lead to other metabolic disorders: type 2 diabetes (DM2), dyslipidemia, and nonalcoholic fatty liver disease (NAFLD). NAFLD may evolve to nonalcoholic steatohepatitis (NASH), and it is related to the development of MS. Lifestyle intervention, physical activity, and weight reduction represent the mainstay of NAFLD therapy. In particular, a catch-up growth reduction could decrease the risk to develop MS and NAFLD. In this paper, we outline clinical and experimental evidences of the association between IUGR, metabolic syndrome, insulin resistance, and NAFLD and discuss on a possible management to avoid the risk of MS in adulthood.
Figures
References
-
- World Health Organization. WHO report: reducing risks, promoting healthy life. Geneva, Switzerland, World Health Organization, 2002.
-
- Barker DJP, Hales CN, Fall CHD, Osmond C, Phipps K, Clark PMS. Type 2 (non-insulin-dependent) diabetes mellitus, hypertension and hyperlipidaemia (syndrome X): relation to reduced fetal growth. Diabetologia. 1993;36(1):62–67. - PubMed
-
- Hattersley AT, Tooke JE. The fetal insulin hypothesis: an alternative explanation of the association of low birthweight with diabetes and vascular disease. Lancet. 1999;353(9166):1789–1792. - PubMed
-
- Haram K, Svendsen E, Myking O. Growth restriction: etiology, maternal and neonatal outcome. A review. Current Women’s Health Reviews. 2007;3(3):145–160.
-
- Valsamakis G, Kanaka-Gantenbein C, Malamitsi-Puchner A, Mastorakos G. Causes of intrauterine growth restriction and the postnatal development of the metabolic syndrome. Annals of the New York Academy of Sciences. 2006;1092:138–147. - PubMed
LinkOut - more resources
Full Text Sources
