

A cost-effectiveness analysis of surgical versus medical management of early pregnancy loss
- PMID: 22192348
- PMCID: PMC3269545
- DOI: 10.1016/j.fertnstert.2011.11.044
A cost-effectiveness analysis of surgical versus medical management of early pregnancy loss
Abstract
Objective: To determine the cost-effectiveness of medical and surgical management of early pregnancy loss.
Design: Analyses of cost, effectiveness, and incremental cost-effectiveness ratios and utilities of a multicenter trial with 652 women with first-trimester pregnancy failure randomized to medical or surgical management.
Setting: Analysis of data from a multicenter trial.
Patient(s): Secondary analysis of a multicenter trial.
Intervention(s): Cost-effectiveness analysis.
Main outcome measure(s): Cost and effectiveness of competing treatment strategies.
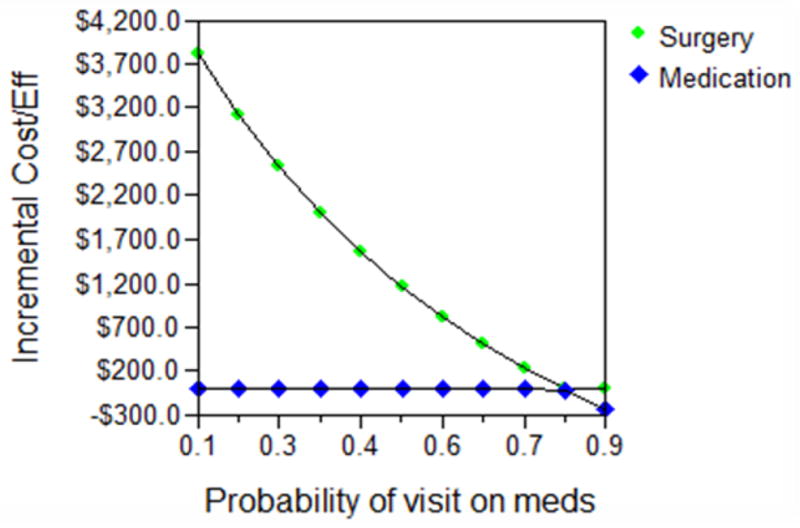
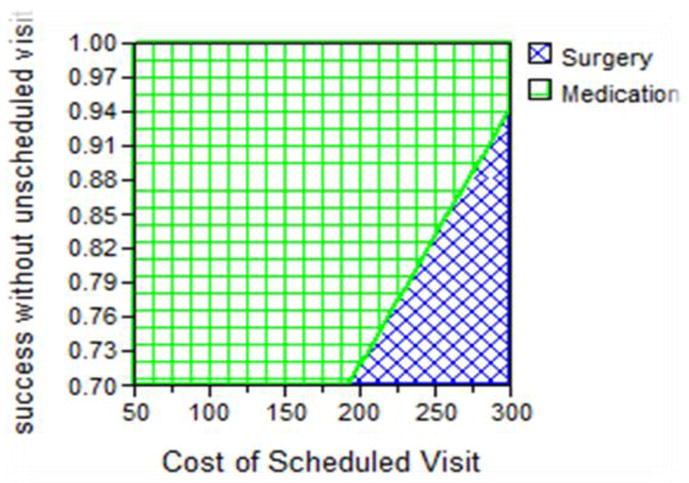
Result(s): Cost analysis of treatment demonstrates an increased cost of US$336 for 13% increased efficacy of surgical management. This analysis was sensitive to the probability of an extra office visit, the cost of the visit, and the probability of success. When the surgical arm is divided into outpatient manual vacuum aspiration (MVA) versus inpatient electric vacuum aspiration (EVA), there is an increased cost of $745 for EVA but a decreased cost of $202 for MVA compared with medical management. In general, MVA was found to be more cost-effective than medical management. For treatment of incomplete or inevitable abortion, medical management was found to be less costly and more efficacious. Utilities studies demonstrated that a patient would need to prefer surgery 14% less than medication for its treatment efficacy to be outweighed by the desire to avoid surgery.
Conclusion(s): Surgical or medical management of early pregnancy failure can be cost effective, depending on the circumstances. Surgery is cost effective and more efficacious when performed in an outpatient setting. For incomplete or inevitable abortion, medical management is cost effective and more efficacious.
Copyright © 2012 American Society for Reproductive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wilcox AJ, Weinberg CR, O’Connor JF, Baird DD, Schlatterer JP, Canfield RE, et al. Incidence of early loss of pregnancy. N Engl J Med. 1988;319(4):189–94. - PubMed
-
- Chen BA, Creinin MD. Medical management of early pregnancy failure: efficacy. Semin Reprod Med. 2008;26(5):411–22. - PubMed
-
- Zhang J, Gilles JM, Barnhart K, Creinin MD, Westhoff C, Frederick MM. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. N Engl J Med. 2005;353(8):761–9. - PubMed
-
- Blumenthal PD, Remsburg RE. A time and cost analysis of the management of incomplete abortion with manual vacuum aspiration. Int J Gynaecol Obstet. 1994;45(3):261–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
