

Correction of postkidney transplant anemia reduces progression of allograft nephropathy
- PMID: 22193388
- PMCID: PMC3269184
- DOI: 10.1681/ASN.2011060546
Correction of postkidney transplant anemia reduces progression of allograft nephropathy
Abstract
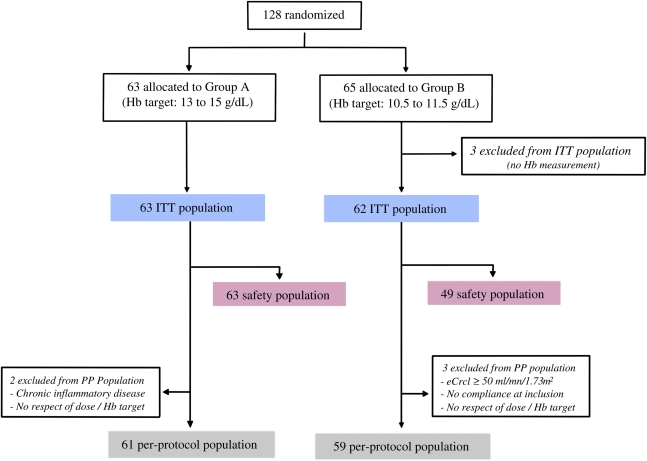
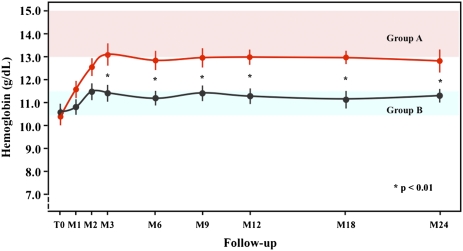
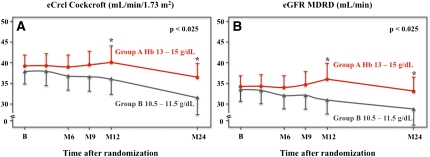
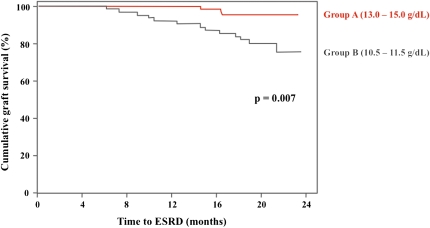
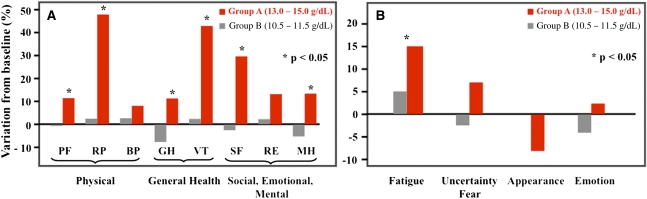
Retrospective studies suggest that chronic allograft nephropathy might progress more rapidly in patients with post-transplant anemia, but whether correction of anemia improves renal outcomes is unknown. An open-label, multicenter, randomized controlled trial investigated the effect of epoetin-β to normalize hemoglobin values (13.0-15.0 g/dl, n=63) compared with partial correction of anemia (10.5-11.5 g/dl, n=62) on progression of nephropathy in transplant recipients with hemoglobin <11.5 g/dl and an estimated creatinine clearance (eCrCl) <50 ml/min per 1.73 m(2). After 2 years, the mean hemoglobin was 12.9 and 11.3 g/dl in the normalization and partial correction groups, respectively (P<0.001). From baseline to year 2, the eCrCl decreased by a mean 2.4 ml/min per 1.73 m(2) in the normalization group compared with 5.9 ml/min per 1.73 m(2) in the partial correction group (P=0.03). Furthermore, fewer patients in the normalization group progressed to ESRD (3 versus 13, P<0.01). Cumulative death-censored graft survival was 95% and 80% in the normalization and partial correction groups, respectively (P<0.01). Complete correction was associated with a significant improvement in quality of life at 6 and 12 months. The number of cardiovascular events was low and similar between groups. In conclusion, this prospective study suggests that targeting hemoglobin values ≥13 g/dl reduces progression of chronic allograft nephropathy in kidney transplant recipients.
Figures
Comment in
-
ESAs in transplant anemia: one size does not "fit all".J Am Soc Nephrol. 2012 Feb;23(2):192-3. doi: 10.1681/ASN.2011121220. Epub 2012 Jan 12. J Am Soc Nephrol. 2012. PMID: 22241895 Free PMC article. No abstract available.
References
-
- Vanrenterghem Y, Ponticelli C, Morales JM, Abramowicz D, Baboolal K, Eklund B, Kliem V, Legendre C, Morais Sarmento ALM, Vincenti F: Prevalence and management of anemia in renal transplant recipients: A European survey. Am J Transplant 3: 835–845, 2003 - PubMed
-
- Winkelmayer WC, Kewalramani R, Rutstein M, Gabardi S, Vonvisger T, Chandraker A: Pharmacoepidemiology of anemia in kidney transplant recipients. J Am Soc Nephrol 15: 1347–1352, 2004 - PubMed
-
- Choukroun G, Deray G, Glotz D, Lebranchu Y, Dussol B, Bourbigot B, Lefrançois N, Cassuto-Viguier E, Toupance O, Hacen C, Lang P, Mazouz H, Martinez F: Incidence and management of anemia in renal transplantation: an observational-French study. Nephrol Ther 4: 575–583, 2008 - PubMed
-
- Molnar MZ, Mucsi I, Macdougall IC, Marsh JE, Yaqoob M, Main J, Courtney AE, Fogarty D, Mikhail A, Choukroun G, Short CD, Covic A, Goldsmith DJ: Prevalence and management of anaemia in renal transplant recipients: Data from ten European centres. Nephron Clin Pract 117: c127–c134, 2011 - PubMed
-
- Kawada N, Moriyama T, Ichimaru N, Imamura R, Matsui I, Takabatake Y, Nagasawa Y, Isaka Y, Kojima Y, Kokado Y, Rakugi H, Imai E, Takahara S: Negative effects of anemia on quality of life and its improvement by complete correction of anemia by administration of recombinant human erythropoietin in posttransplant patients. Clin Exp Nephrol 13: 355–360, 2009 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
