

Biologic imaging of head and neck cancer: the present and the future
- PMID: 22194364
- PMCID: PMC8050463
- DOI: 10.3174/ajnr.A2535
Biologic imaging of head and neck cancer: the present and the future
Abstract
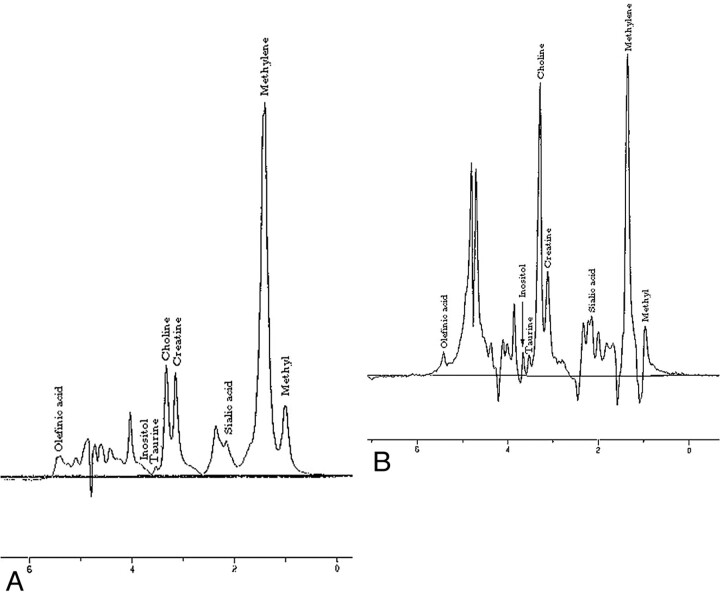
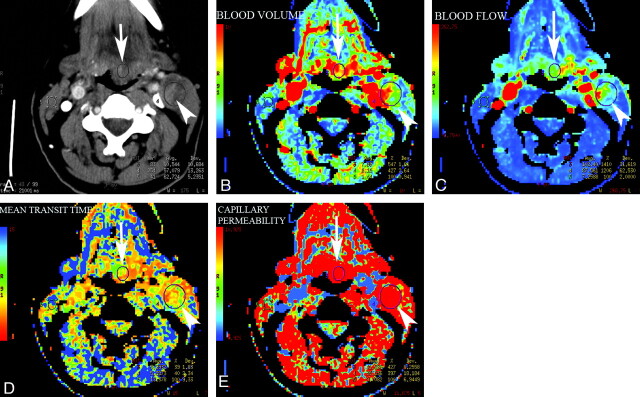
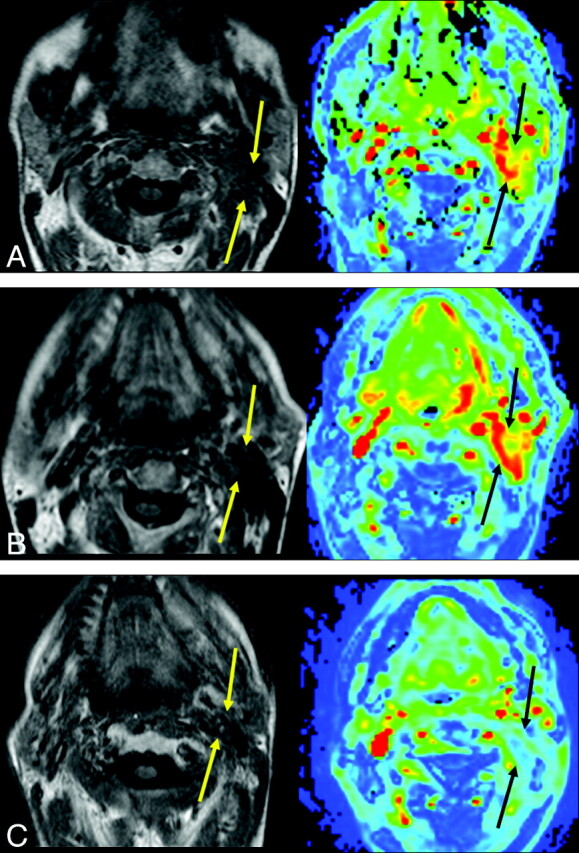
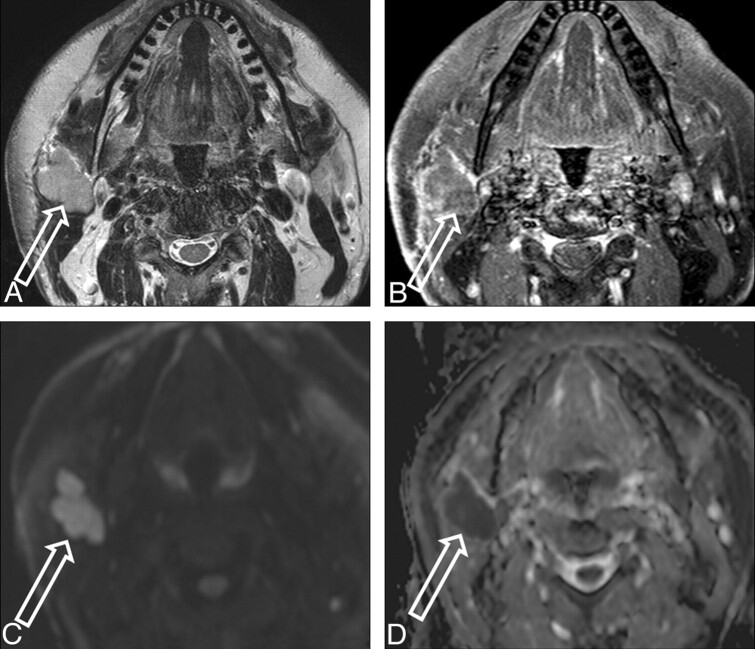
While anatomic imaging (CT and MR imaging) of HNC is focused on diagnosing and/or characterizing the disease, defining its local extent, and evaluating distant spread, accurate assessment of the biologic status of the cancer (cellularity, growth rate, response to nonsurgical chemoradiation therapy, and so forth) can be invaluable for prognostication, planning therapy, and follow-up of lesions after therapy. The combination of anatomic and biologic imaging techniques can thus provide a more comprehensive evaluation of the patient. The purpose of this work was to review the present and future clinical applications of advanced biologic imaging techniques in HNC evaluation and management. As part of the biologic imaging array, we discuss MR spectroscopy, diffusion and perfusion MR imaging, CTP, and FDG-PET scanning and conclude with exciting developments that hold promise in assessment of tumor hypoxia and neoangiogenesis.
Figures
References
-
- American Cancer Society. www.cancer.org. Accessed October 28, 2007
-
- Delikatny EJ, Russell P, Hunter JC, et al. . Proton MR and human cervical neoplasia: ex vivo spectroscopy allows distinction of invasive carcinoma of the cervix from carcinoma in situ and other preinvasive lesions. Radiology 1993;188: 791–96 - PubMed
-
- Gill SS, Thomas DG, Van Bruggen N, et al. . Proton MR spectroscopy of intracranial tumours: in vivo and in vitro studies. J Comput Assist Tomogr 1990;14: 497–504 - PubMed
-
- Negendank WG, Brown TR, Evelhoch JL, et al. . Proceedings of a National Cancer Institute workshop: MR spectroscopy and tumor cell biology. Radiology 1992;185: 875–83 - PubMed
-
- Shah GV, Gandhi D, Mukherji SK. Magnetic resonance spectroscopy of head and neck neoplasms. Top Magn Reson Imaging 2004;15: 87–94 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials