

Closed Meningo(encephalo)cele: a new feature in Hunter syndrome
- PMID: 22194384
- PMCID: PMC7968812
- DOI: 10.3174/ajnr.A2867
Closed Meningo(encephalo)cele: a new feature in Hunter syndrome
Abstract
Background and purpose: Hunter syndrome (MPS type II) is a rare X-linked recessive disease caused by lysosomal enzyme iduronate-2-sulfatase deficiency, characterized by frequent and variable brain and skull involvement. Our objective was determine the frequency of closed cephaloceles in a large cohort of subjects affected with Hunter syndrome and to investigate possible correlations with clinical and neuroradiologic findings.
Materials and methods: Brain MR imaging of 33 patients (32 males and 1 female, age range 2.5-30.8 years, mean age 10.4 years) affected with Hunter syndrome were retrospectively evaluated. Eleven (age range 3.6-30.8 years; mean age 15.1) presented with an "attenuated" phenotype, while 22 (age range 2.5-19.1 years; mean age 8.2) had a "severe" phenotype.
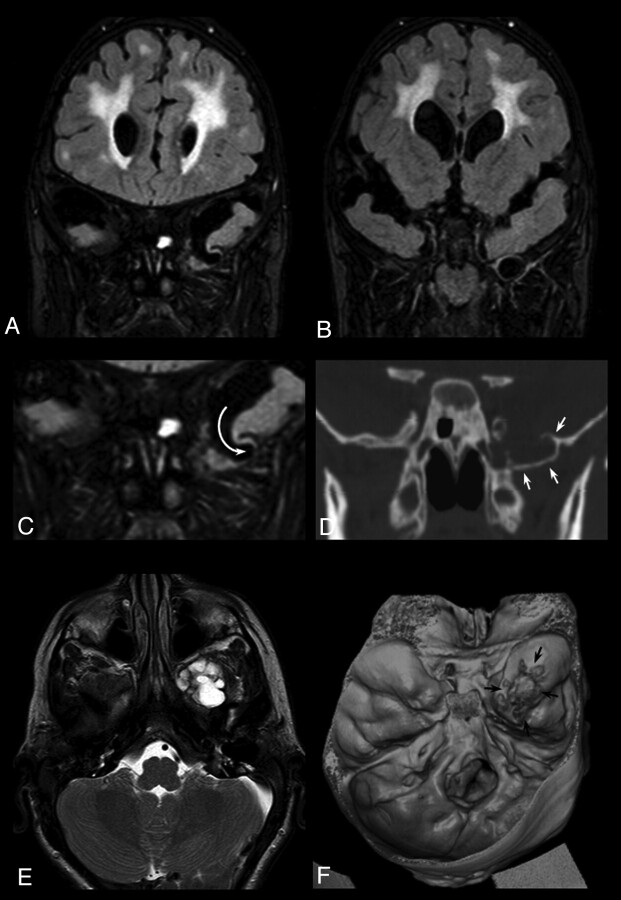
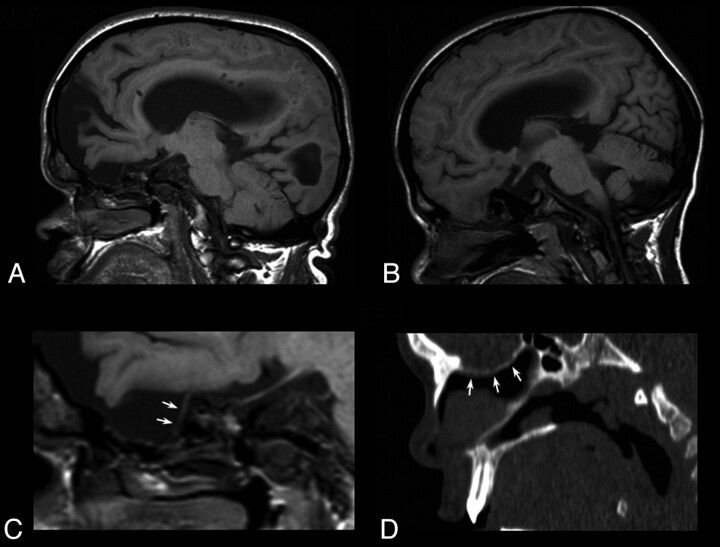
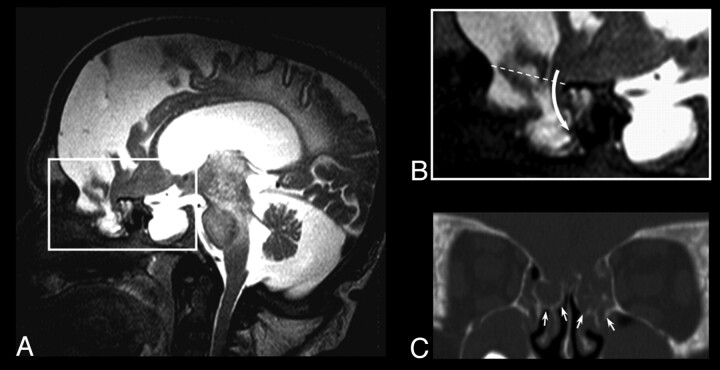
Results: A closed cephalocele was detected in 9/33 patients (27%) at the level of anterior and middle fossa in 6 and 3 cases, respectively; 6/9 subjects were affected with the attenuated phenotype and 1/9 suffered from epilepsy. Closed cephaloceles did not show a significant association with other brain and spine MR imaging features of Hunter disease, such as enlargement of perivascular spaces, cisterna magna, pituitary sella, ventricles and subarachnoid spaces, craniosynostosis, dens hypoplasia, white matter abnormalities, spinal stenosis due to periodontoid cap, platyspondylia, or intervertebral disk anomalies.
Conclusions: Closed cephaloceles are frequent in Hunter syndrome and should be considered a neuroradiologic feature of this disease.
Figures
Similar articles
-
Brain and spine MRI features of Hunter disease: frequency, natural evolution and response to therapy.J Inherit Metab Dis. 2011 Jun;34(3):763-80. doi: 10.1007/s10545-011-9317-5. Epub 2011 Apr 5. J Inherit Metab Dis. 2011. PMID: 21465231
-
Cervical spine MRI findings in patients with Mucopolysaccharidosis type II.Pediatr Neurosurg. 2015;50(1):26-30. doi: 10.1159/000371658. Epub 2015 Feb 25. Pediatr Neurosurg. 2015. PMID: 25721852
-
Hunter syndrome in an 11-year old girl on enzyme replacement therapy with idursulfase: brain magnetic resonance imaging features and evolution.J Inherit Metab Dis. 2010 Dec;33 Suppl 3:S67-72. doi: 10.1007/s10545-009-9023-8. Epub 2010 Jan 6. J Inherit Metab Dis. 2010. PMID: 20052546
-
Mucopolysaccharidosis type II (Hunter syndrome): a clinical review and recommendations for treatment in the era of enzyme replacement therapy.Eur J Pediatr. 2008 Mar;167(3):267-77. doi: 10.1007/s00431-007-0635-4. Epub 2007 Nov 23. Eur J Pediatr. 2008. PMID: 18038146 Free PMC article. Review.
-
Multidisciplinary management of Hunter syndrome.Pediatrics. 2009 Dec;124(6):e1228-39. doi: 10.1542/peds.2008-0999. Epub 2009 Nov 9. Pediatrics. 2009. PMID: 19901005 Review.
Cited by
-
Imaging findings of mucopolysaccharidoses: a pictorial review.Insights Imaging. 2013 Aug;4(4):443-59. doi: 10.1007/s13244-013-0246-8. Epub 2013 May 5. Insights Imaging. 2013. PMID: 23645566 Free PMC article.
-
Targeting Neurological Aspects of Mucopolysaccharidosis Type II: Enzyme Replacement Therapy and Beyond.BioDrugs. 2024 Sep;38(5):639-655. doi: 10.1007/s40259-024-00675-0. Epub 2024 Aug 23. BioDrugs. 2024. PMID: 39177874 Free PMC article. Review.
-
Brain Proteomic Profiling in Intractable Epilepsy Caused by TSC1 Truncating Mutations: A Small Sample Study.Front Neurol. 2020 May 29;11:475. doi: 10.3389/fneur.2020.00475. eCollection 2020. Front Neurol. 2020. PMID: 32655475 Free PMC article.
-
Chiari 1 malformation and holocord syringomyelia in hunter syndrome.JIMD Rep. 2014;12:31-5. doi: 10.1007/8904_2013_241. Epub 2013 Jul 2. JIMD Rep. 2014. PMID: 23818180 Free PMC article.
-
Mucopolysaccharidoses: overview of neuroimaging manifestations.Pediatr Radiol. 2018 Sep;48(10):1503-1520. doi: 10.1007/s00247-018-4139-3. Epub 2018 May 11. Pediatr Radiol. 2018. PMID: 29752520 Review.
References
-
- Martin R, Beck M, Eng C, et al. . Recognition and diagnosis of mucopolysaccharidosis II (Hunter Syndrome). Pediatrics 2008;121:e377–86 - PubMed
-
- Muenzer J, Beck M, Eng CM, et al. . Multidisciplinary management of Hunter syndrome. Pediatrics 2009;124:e1228–39 - PubMed
-
- Al Sawaf S, Mayatepek E, Hoffmann B. Neurological findings in Hunter disease: pathology and possible therapeutic effects reviewed. J Inherit Metab Dis 2008;31:473–80 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous