

Lung manifestations in an autopsy-based series of pulmonary or disseminated nontuberculous mycobacterial disease
- PMID: 22194586
- PMCID: PMC3342780
- DOI: 10.1378/chest.11-0425
Lung manifestations in an autopsy-based series of pulmonary or disseminated nontuberculous mycobacterial disease
Abstract
Background: Comparisons of lung manifestations in primary pulmonary vs disseminated nontuberculous mycobacterial disease have not been well described. The clinical, histopathologic, and radiologic disease manifestations of primary pulmonary or disseminated nontuberculous mycobacterial disease were compared in an autopsy series.
Methods: Medical and microbiologic records, autopsy reports, histopathologic slides of the lungs, and chest CT scans were reviewed on patients at the National Institutes of Health with nontuberculous mycobacterial disease who died between 1996 and 2010.
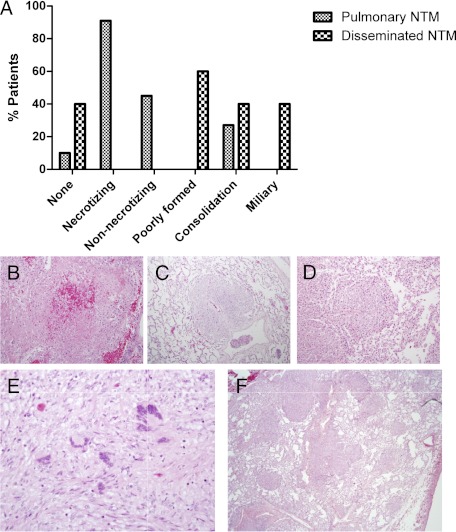
Results: The 11 patients with primary pulmonary nontuberculous mycobacterial disease were predominantly female (n = 9), with symptom onset at median 50 (range 35, 71) years and time from onset until death of 12 (3, 34) years. Bronchiectasis with cavity formation and necrotizing bronchocentric granulomatous inflammation predominated but extrapulmonary infection was absent. The five patients with disseminated disease and systemic immune defects were all men with age at onset of 2 (0.33, 33) years and time from onset of disease until death of 9 (1, 31) years. Miliary nodules and/or consolidation with poorly formed granulomatous inflammation were noted in the three disseminated patients with mycobacterial lung involvement. Significant extrapulmonary infection was noted in all five with a relative paucity of lung findings.
Conclusions: Nontuberculous mycobacteria can cause progressive, fatal disease. Primary pulmonary disease is bronchocentric and lacks extrathoracic infection consistent with impaired airway surface defenses. In contrast, fatal disseminated infections involving the lung have hematogenous spread, extensive extrathoracic disease, and a distinct pulmonary histopathology consistent with systemic immune dysfunction.
Figures
References
-
- Griffith DE, Aksamit T, Brown-Elliott BA, et al. ATS Mycobacterial Diseases Subcommittee American Thoracic Society Infectious Disease Society of America An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases [erratum published in: Am J Respir Crit Care Med. 2007;175(7):744-745] Am J Respir Crit Care Med. 2007;175(4):367–416. - PubMed
-
- Sexton P, Harrison AC. Susceptibility to nontuberculous mycobacterial lung disease. Eur Respir J. 2008;31(6):1322–1333. - PubMed
-
- Afessa B, Green W, Chiao J, Frederick W. Pulmonary complications of HIV infection: autopsy findings. Chest. 1998;113(5):1225–1229. - PubMed
-
- Dorman SE, Picard C, Lammas D, et al. Clinical features of dominant and recessive interferon gamma receptor 1 deficiencies. Lancet. 2004;364(9451):2113–2121. - PubMed
-
- Orange JS, Jain A, Ballas ZK, Schneider LC, Geha RS, Bonilla FA. The presentation and natural history of immunodeficiency caused by nuclear factor kappaB essential modulator mutation. J Allergy Clin Immunol. 2004;113(4):725–733. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
