

Frailty and respiratory impairment in older persons
- PMID: 22195532
- PMCID: PMC3246194
- DOI: 10.1016/j.amjmed.2011.06.024
Frailty and respiratory impairment in older persons
Abstract
Background: Among older persons, the association between frailty and spirometry-confirmed respiratory impairment has not been evaluated yet.
Methods: By using data on white participants aged 65 to 80 years (Cardiovascular Health Study, N=3578), we evaluated cross-sectional and longitudinal associations between frailty and respiratory impairment, including their combined effect on mortality. Baseline assessments included frailty status (Fried phenotype: non-frail, pre-frail, and frail) and spirometry. Outcomes included development of frailty features (pre-frail or frail) at year 3 and respiratory impairment (airflow limitation or restrictive pattern) at year 4, and death (median follow-up, 13.2 years).
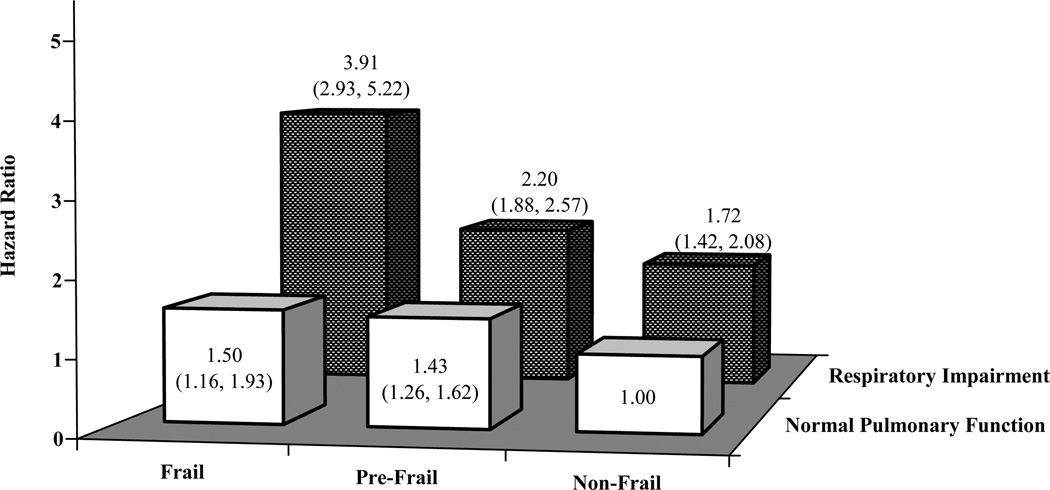
Results: At baseline, 48.3% of participants were pre-frail, 5.8% of participants were frail, 13.8% of participants had airflow limitation, and 9.3% of participants had restrictive pattern; 46.1% of participants subsequently died. At baseline, pre-frail and frail were cross-sectionally associated with airflow limitation (adjusted odds ratio [OR], 1.62; 95% confidence interval [CI], 1.29-2.04 and adjusted OR 1.88; 95% CI, 1.15-3.09) and restrictive pattern (adjusted OR, 1.80; 95% CI, 1.37-2.36 and adjusted OR, 3.05; 95% CI, 1.91-4.88), respectively. Longitudinally, participants with baseline frailty features had an increased likelihood of developing respiratory impairment (adjusted OR, 1.42; 95% CI, 1.11-1.82). Conversely, participants with baseline respiratory impairment had an increased likelihood of developing frailty features (adjusted OR, 1.58; 95% CI, 1.17-2.13). Mortality was highest among participants who were frail and had respiratory impairment (adjusted hazard ratio, 3.91; 95% CI, 2.93-5.22), compared with those who were non-frail and had no respiratory impairment.
Conclusion: Frailty and respiratory impairment are strongly associated with one another and substantially increase the risk of death when both are present. Establishing these associations may inform interventions designed to reverse or prevent the progression of either condition and to reduce adverse outcomes.
Published by Elsevier Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Fried L, Tangen M, Walston J, et al. Frailty in older adults: Evidence for a phenotype. J Gerontol Med Sci. 2001;56A:M146–M156. - PubMed
-
- Rockwood K, Howlett S, MacKnight C, et al. Prevalence, attributes, and outcomes of fitness and frailty in community-dwelling older adults: report from the Canadian study of health and aging. J Gerontol Med Sci. 2004;59A:1310–1317. - PubMed
-
- Boyd CM, Xue Q-L, Simpson CF, et al. Frailty, hospitalization, and progression of disability in a cohort of disabled older women. Am J Med. 2005;118:1225–1231. - PubMed
-
- CDC. Second National Report on Human Exposure to Environmental Chemicals: Tobacco Smoke. Morb Mortal Wkly Rep. 2002;51:300–303.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
