

Results of proximal arch replacement using deep hypothermia for circulatory arrest: is moderate hypothermia really justifiable?
- PMID: 22196653
- PMCID: PMC3732664
Results of proximal arch replacement using deep hypothermia for circulatory arrest: is moderate hypothermia really justifiable?
Abstract
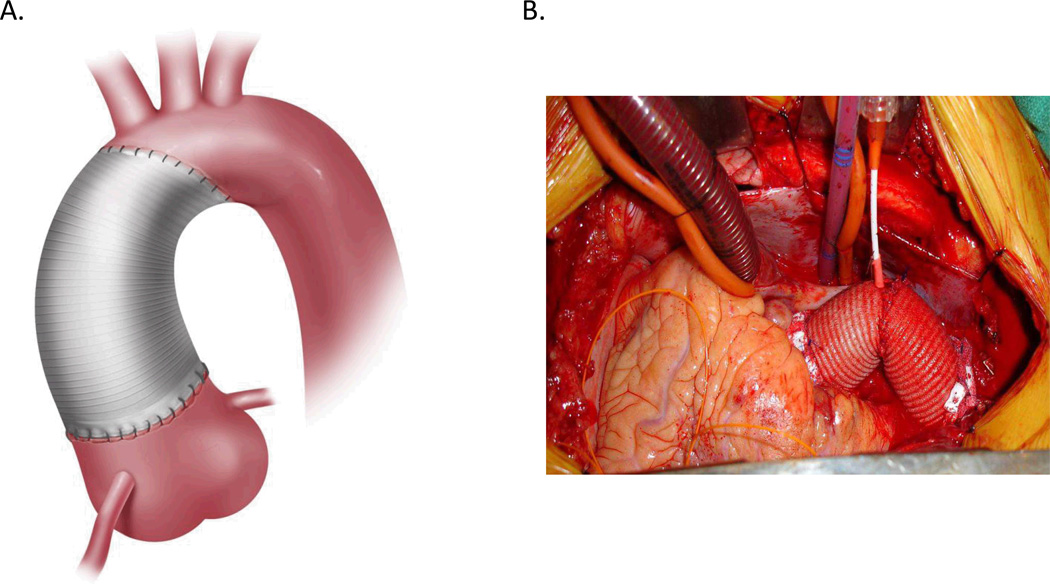
The use of selective cerebral perfusion with warmer temperatures during circulatory arrest has been increasingly used for arch replacement over concerns regarding the safety of deep hypothermic circulatory arrest (DHCA). However, little data actually exist on outcomes after arch replacement and DHCA. This study examines modern results with DHCA for proximal arch replacement to provide a benchmark for comparison against outcomes with lesser degrees of hypothermia. Between July 2005 and June 2010, 245 proximal arch replacements ("hemiarch") were performed using deep hypothermia; mean minimum core and nasopharyngeal temperatures were 18.0 ± 2.1°C and 14.1 ± 1.6°C, respectively. Adjunctive cerebral perfusion was used in all cases. Concomitant ascending aortic replacement was performed in 41 per cent, ascending plus aortic valve replacement in 23 per cent, and aortic root replacement in 32 per cent. Mean age was 58 ± 14 years; 36 per cent procedures were urgent/emergent. Mean duration of DHCA was 20.4 ± 6.2 minutes. Thirty-day/in-hospital mortality was 2.9 per cent. Rates of stroke, renal failure, and respiratory failure were 4.1 per cent (0.8% for elective cases), 1.2 per cent, and 0.4 per cent, respectively. Deep hypothermia with adjunctive cerebral perfusion for circulatory arrest during proximal arch replacement affords excellent neurologic as well as nonneurologic outcomes. Centers using lesser degrees of hypothermia for arch surgery, the safety of which remains unproven, should ensure comparable results.
Figures
References
-
- Bachet J, Guilmet D, Goudot B, et al. Antegrade cerebral perfusion with cold blood: A 13-year experience. Ann Thorac Surg. 1999;67:1874–1878. discussion 1891-1874. - PubMed
-
- Cooley DA, Mahaffey DE, De Bakey ME. Total excision of the aortic arch for aneurysm. Surg Gynecol Obstet. 1955;101:667–672. - PubMed
-
- Crawford ES, Saleh SA, Schuessler JS. Treatment of aneurysm of transverse aortic arch. J Thorac Cardiovasc Surg. 1979;78:383–393. - PubMed
-
- Griepp RB, Stinson EB, Hollingsworth JF, Buehler D. Prosthetic replacement of the aortic arch. J Thorac Cardiovasc Surg. 1975;70:1051–1063. - PubMed
-
- Halkos ME, Kerendi F, Myung R, et al. Selective antegrade cerebral perfusion via right axillary artery cannulation reduces morbidity and mortality after proximal aortic surgery. J Thorac Cardiovasc Surg. 2009;138:1081–1089. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources